

The Role of Inflammation in the Pathophysiology of Heart Failure
- PMID: 40710370
- PMCID: PMC12293573
- DOI: 10.3390/cells14141117
The Role of Inflammation in the Pathophysiology of Heart Failure
Abstract
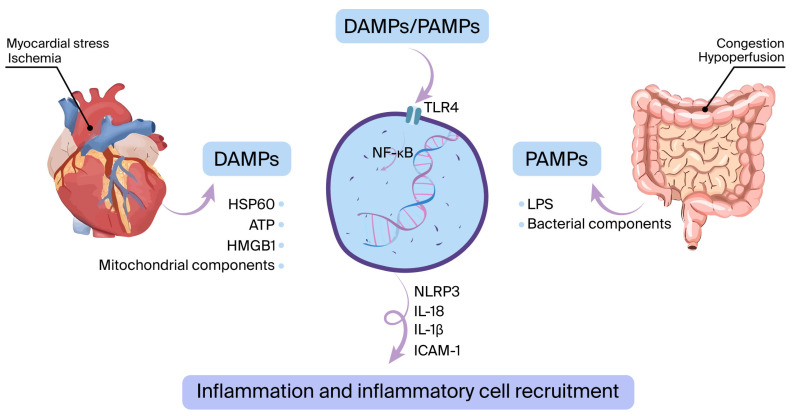
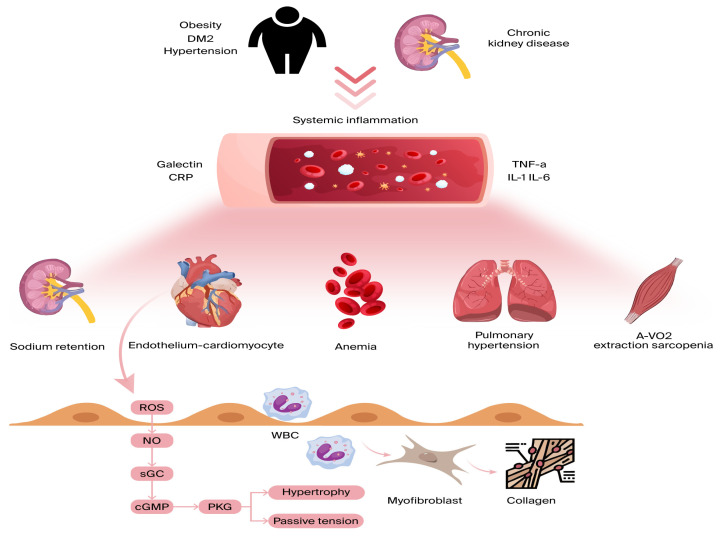
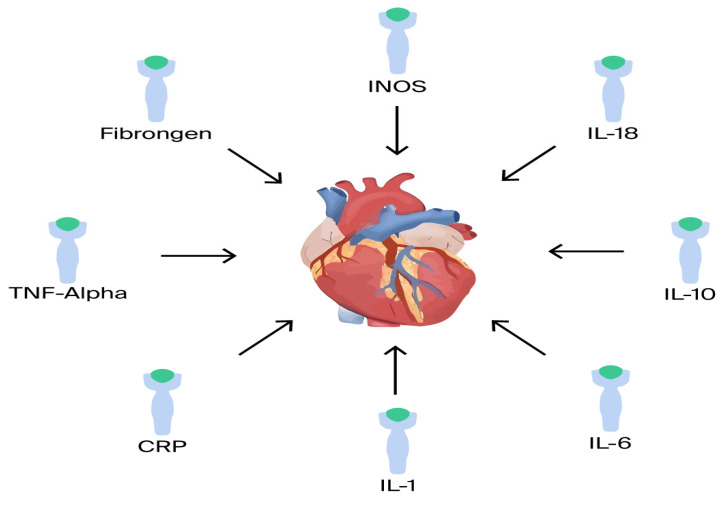
Heart failure (HF), a prevalent global health issue characterized by the heart's impaired ability to pump or fill blood, affects millions worldwide and continues to pose significant challenges despite advancements in treatment. This review delves into the critical and increasingly recognized role of inflammation in the development and progression of this complex syndrome. While the incidence of HF has seen a decline in some regions due to improved cardiac care, its overall prevalence is rising, particularly among younger adults and those with heart failure with a preserved ejection fraction (HFpEF). Given the persistently high rates of hospitalization and mortality associated with HF, understanding the underlying mechanisms, including the contribution of inflammation, is crucial for identifying novel therapeutic strategies. Inflammation in heart failure is a multifaceted process involving the activation of the immune system, both innate and adaptive, and encompasses various mechanisms such as the release of pro-inflammatory mediators, endothelial dysfunction, and neurohormonal activation. Myocardial damage triggers the innate immune response, while humoral immunity and chronic systemic inflammation, often linked to cardiovascular risk factors and autoimmune diseases, also play significant roles. Notably, heart failure and inflammation have a reciprocal relationship, with HF itself contributing to inflammatory processes within the cardiac tissue and systemically. Understanding these intricate pathways, including the involvement of specific immune cells and molecular mediators, is essential for comprehending the pathogenesis of heart failure and exploring potential therapeutic interventions. The review further examines various inflammatory biomarkers that have been implicated in heart failure, such as cytokines (including TNF-α and IL-1) and C-reactive protein (CRP). While these markers often correlate with the severity and prognosis of HF, clinical trials targeting specific inflammatory mediators have largely yielded disappointing results, highlighting the complexity of the inflammatory response in this context. The exploration of these biomarkers and the challenges encountered in translating anti-inflammatory strategies into effective treatments underscore the need for continued research to unravel the precise role of inflammation across different HF subtypes and to develop more targeted and effective anti-inflammatory therapies.
Keywords: HErEF; HFpEF; epidemiology; heart failure; inflammation; pathophysiology.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Systemic Inflammatory Response Syndrome.2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449 Free Books & Documents.
-
A Comprehensive Review: Unraveling the Role of Inflammation in the Etiology of Heart Failure.Heart Fail Rev. 2025 Sep;30(5):931-954. doi: 10.1007/s10741-025-10519-w. Epub 2025 May 14. Heart Fail Rev. 2025. PMID: 40360833 Free PMC article. Review.
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2020 Jan 9;1(1):CD011535. doi: 10.1002/14651858.CD011535.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 19;4:CD011535. doi: 10.1002/14651858.CD011535.pub4. PMID: 31917873 Free PMC article. Updated.
References
-
- Bozkurt B., Ahmad T., Alexander K.M., Baker W.L., Bosak K., Breathett K., Fonarow G.C., Heidenreich P., Ho J.E., Hsich E., et al. Heart Failure Epidemiology and Outcomes Statistics: A Report of the Heart Failure Society of America. J. Card. Fail. 2023;29:1412–1451. doi: 10.1016/j.cardfail.2023.07.006. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
