

Artificial Intelligence Dystocia Algorithm (AIDA) as a Decision Support System in Transverse Fetal Head Position
- PMID: 40710610
- PMCID: PMC12295838
- DOI: 10.3390/jimaging11070223
Artificial Intelligence Dystocia Algorithm (AIDA) as a Decision Support System in Transverse Fetal Head Position
Abstract
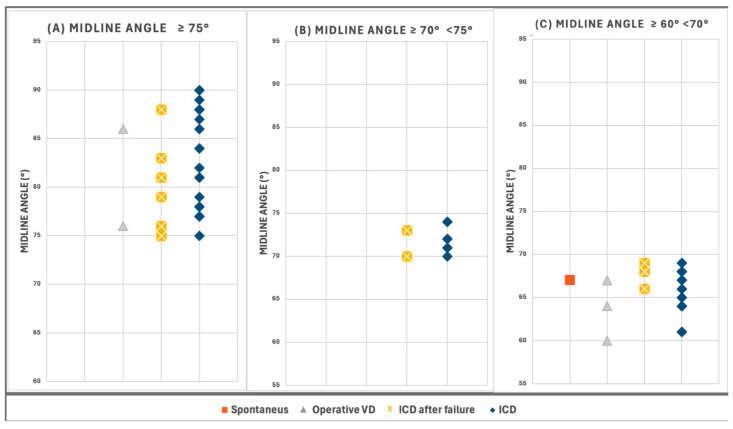
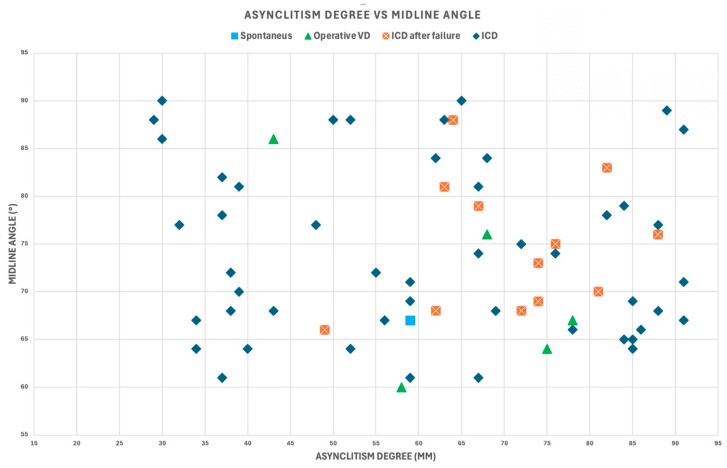
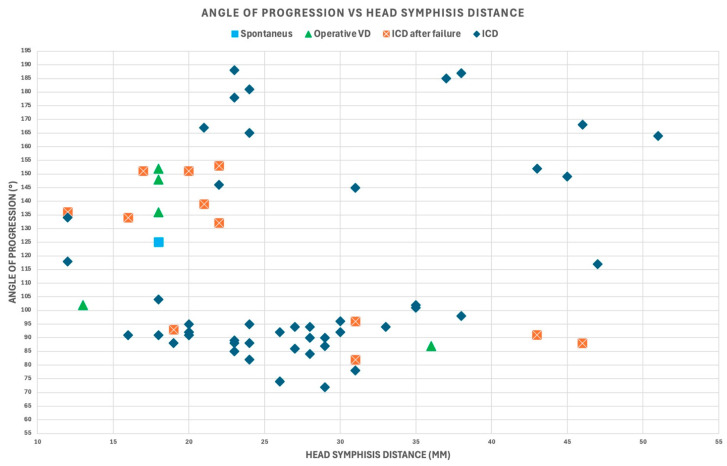
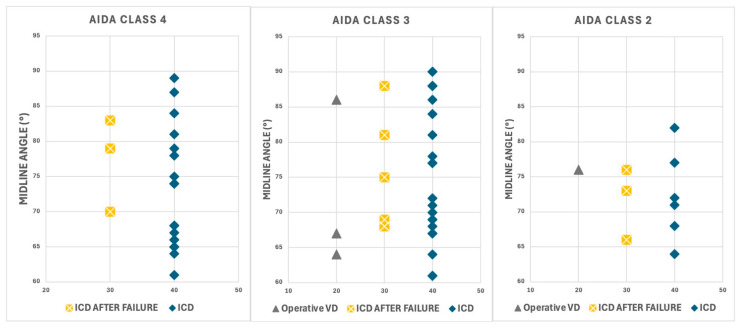
Transverse fetal head position during labor is associated with increased rates of operative deliveries and cesarean sections. Traditional assessment methods rely on digital examination, which can be inaccurate in cases of prolonged labor. Intrapartum ultrasound offers improved diagnostic capabilities, but standardized interpretation frameworks are needed. This study aimed to evaluate the significance of appropriate assessment and management of transverse fetal head position during labor, with particular emphasis on the correlation between geometric parameters and delivery outcomes. Additionally, the investigation analyzed the potential role of Artificial Intelligence Dystocia Algorithm (AIDA) as an innovative decision support system in standardizing diagnostic approaches and optimizing clinical decision-making in cases of fetal malposition. This investigation was conducted as a focused secondary analysis of data originally collected for the development and validation of the Artificial Intelligence Dystocia Algorithm (AIDA). The study examined 66 cases of transverse fetal head position from a cohort of 135 nulliparous women with prolonged second-stage labor across three Italian hospitals. Cases were stratified by Midline Angle (MLA) measurements into classic transverse (≥75°), near-transverse (70-74°), and transitional (60-69°) positions. Four geometric parameters (Angle of Progression, Head-Symphysis Distance, Midline Angle, and Asynclitism Degree) were evaluated using the AIDA classification system. The predictive capabilities of three machine learning algorithms (Support Vector Machine, Random Forest, and Multilayer Perceptron) were assessed, and delivery outcomes were analyzed. The AIDA system successfully categorized labor dystocia into five distinct classes, with strong predictive value for delivery outcomes. A clear gradient of cesarean delivery risk was observed across the spectrum of transverse positions (100%, 93.1%, and 85.7% for near-transverse, classic transverse, and transitional positions, respectively). All cases classified as AIDA Class 4 required cesarean delivery regardless of the specific MLA value. Machine learning algorithms demonstrated high predictive accuracy, with Random Forest achieving 95.5% overall accuracy across the study cohort. The presence of concurrent asynclitism with transverse position was associated with particularly high rates of cesarean delivery. Among the seven cases that achieved vaginal delivery despite transverse positioning, none belonged to the classic transverse positions group, and five (71.4%) exhibited at least one parameter classified as favorable. The integration of artificial intelligence through AIDA as a decision support system, combined with intrapartum ultrasound, offered a promising approach for objective assessment and management of transverse fetal head position. The AIDA classification system's integration of multiple geometric parameters, with particular emphasis on precise Midline Angle (MLA) measurement in degrees, provided superior predictive capability for delivery outcomes compared to qualitative position assessment alone. This multidimensional approach enabled more personalized and evidence-based management of malpositions during labor, potentially reducing unnecessary interventions while identifying cases where expectant management might be futile. Further prospective studies are needed to validate the predictive capability of this decision support system and its impact on clinical decision-making in real-time labor management.
Keywords: Artificial Intelligence Dystocia Algorithm (AIDA); cesarean delivery; decision support system; intrapartum ultrasound; labor dystocia; machine learning; midline angle; occiput transverse position; transverse fetal head position.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
AIDA (Artificial Intelligence Dystocia Algorithm) in Prolonged Dystocic Labor: Focus on Asynclitism Degree.J Imaging. 2024 Aug 9;10(8):194. doi: 10.3390/jimaging10080194. J Imaging. 2024. PMID: 39194983 Free PMC article.
-
Maternal and neonatal outcomes of elective induction of labor.Evid Rep Technol Assess (Full Rep). 2009 Mar;(176):1-257. Evid Rep Technol Assess (Full Rep). 2009. PMID: 19408970 Free PMC article.
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Prophylactic manual rotation of the fetal head (manual rotation alone) to reduce operative delivery and complications for mother and babies.Cochrane Database Syst Rev. 2025 Jul 18;7(7):CD009298. doi: 10.1002/14651858.CD009298.pub3. Cochrane Database Syst Rev. 2025. PMID: 40678975
-
Does the Presence of Missing Data Affect the Performance of the SORG Machine-learning Algorithm for Patients With Spinal Metastasis? Development of an Internet Application Algorithm.Clin Orthop Relat Res. 2024 Jan 1;482(1):143-157. doi: 10.1097/CORR.0000000000002706. Epub 2023 Jun 12. Clin Orthop Relat Res. 2024. PMID: 37306629 Free PMC article.
References
-
- Yano E., Sayama S., Iriyama T., Ariyoshi Y., Akiba N., Ichinose M., Toshimitsu M., Seyama T., Kumasawa K., Nakayama T., et al. Prediction of spontaneous vaginal delivery in the prolonged second stage using the delta angle of progression. Am. J. Obstet. Gynecol. MFM. 2024;6:101403. doi: 10.1016/j.ajogmf.2024.101403. - DOI - PubMed
LinkOut - more resources
Full Text Sources
