

Comprehensive observations and multidisciplinary approaches (COMA) in the management of unconscious patients: a prospective high fidelity simulation study
- PMID: 40711621
- PMCID: PMC12296809
- DOI: 10.1007/s00415-025-13228-4
Comprehensive observations and multidisciplinary approaches (COMA) in the management of unconscious patients: a prospective high fidelity simulation study
Abstract
Background: Managing patients with coma of unknown etiology presents a challenge requiring rapid, structured assessment. We aimed to examine how physicians from different specialties manage patients with coma of unknown etiology and adhere to recommendations in a highly standardized scenario.
Methods: Prospective high-fidelity simulation study conducted at an academic simulation center involving 50 physicians from acute care (38%), internal medicine (36%), and neurology (26%). Participants were confronted with a standardized coma scenario. Performance was assessed for adherence to expert-recommended clinical assessments (primary endpoints) and timing of interventions, such as airway protection, oxygen administration, toxicological screening, and self-evaluation (secondary endpoints).
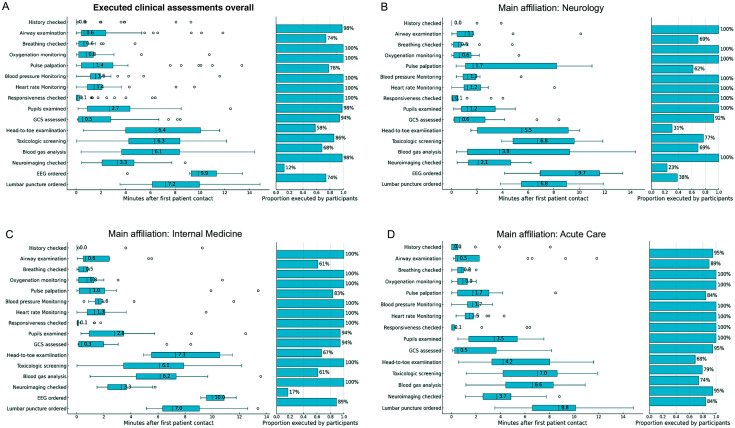
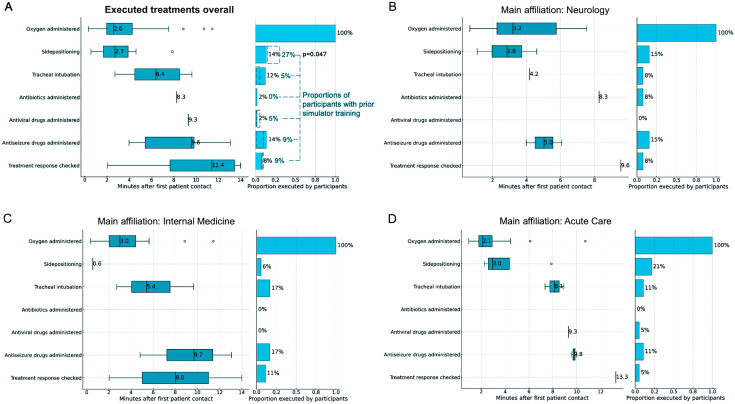
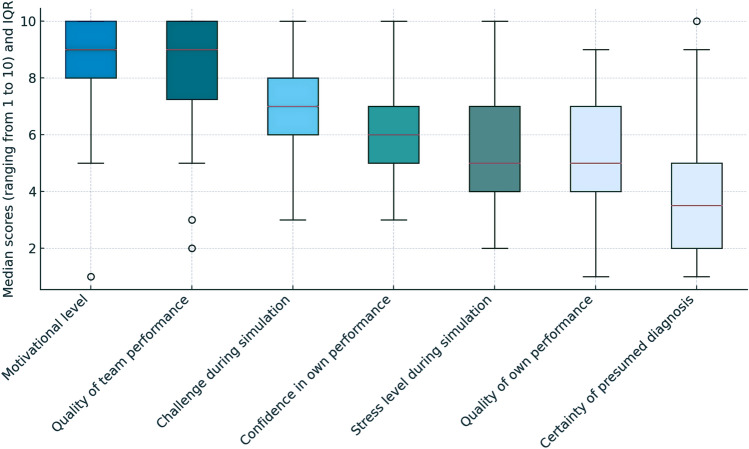
Results: All participants recognized coma; 80% assessed the Glasgow Coma Scale, with 40% quantifying it correctly. 20% completed ABCDE assessments, with 66% performing head-to-toe examinations. Airway inspection was conducted by 89% of acute care physicians, 70% of neurologists, and 60% of internists. A median of 4 ancillary tests were ordered, mostly neuroimaging (98%) and toxicological screening (86%), while rare toxin screening (2%) and EEG (12%) were scarce. Oxygen was universally administered (100%), but treatment response was rarely checked (8%). Side-positioning for airway protection was infrequent (21% acute care, 15% neurology, 6% internal medicine), while intubation was more commonly ordered by internists (17%). Prior simulator training improved side-positioning rates (27% vs. 4%, p = 0.047). Self-evaluations showed high motivation (median 8/10) but moderate confidence (5/10).
Conclusions: This study highlights specialty-specific differences, misconceptions, and gaps in managing coma of unknown etiology, including inconsistent diagnostic workup and missed treatments, emphasizing the need for guidelines, standardized care and training.
Registration: ClinicalTrials.gov registry (ID NCT06265168).
Keywords: Coma; Neurocritical care; Prospective study; Simulator study.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: L. Nüesch reports no disclosures relevant to the manuscript. K. Tisljar reports no disclosures relevant to the manuscript. S. Berger reports no disclosures relevant to the manuscript. G.M. De Marchis was or is supported by the Swiss National Science Foundation; Science Funds [Wissenschaftsfonds] of the University Hospital Basel and University of Basel; Bangerter-Rhyner-Stiftung; Swisslife Jubiläumsstiftung for Medical Research; Swiss Neurological Society; Fondazione Dr. Ettore Balli; De Quervain research grant; Thermo Fisher GmbH. He received travel honoraria by Bayer and speaker honoraria by Medtronic and BMS/Pfizer. T.D. Dittrich was or is supported by the Swiss Heart Foundation, the science funds of the University Hospital Basel, and the Research Fund for excellent young researchers of the University of Basel. He holds shares from Johnson & Johnson, Roche, Lilly, Bristol-Myers Squibb, Merck, and Novo Nordisk. S. Bassetti reports no disclosures relevant to the manuscript. R. Bingisser is editor of medstandards.com, a symptom-based medical decision-support tool licensed to 150 European hospitals, owned by the University Hospital Basel. S. Hunziker is supported by the Swiss National Foundation (SNF) (Ref 10001C_192850/1 and 10531C_182422), the Bangerter-Rhyner Foundation (8472/HEG-DSV), and the Swiss Society of General Internal Medicine (SSGIM). S. Marsch reports no disclosures relevant to the manuscript. R. Sutter received research grants from the Swiss National Foundation (No 320030_169379), the Research Fund of the University Basel, the Scientific Society Basel, and the Gottfried Julia Bangerter-Rhyner Foundation. He received personal grants from UCB-pharma and holds stocks from Alcon, Johnson & Johnson, Novartis, and Roche. Use of artificial intelligence-assisted technologies: The large language model (ChatGPT-4omni, OpenAI, San Francisco, USA) was used to paraphrase and summarize some of the manuscript’s content. After using this application, the authors further edited the content as needed and verified its accuracy. Ethical Standard Statement: The study has been approved by the appropriate local ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants consented to participate in written form.
Figures
Similar articles
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Head impulse, nystagmus, and test of skew examination for diagnosing central causes of acute vestibular syndrome.Cochrane Database Syst Rev. 2023 Nov 2;11(11):CD015089. doi: 10.1002/14651858.CD015089.pub2. Cochrane Database Syst Rev. 2023. PMID: 37916744 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Heliox for croup in children.Cochrane Database Syst Rev. 2021 Aug 16;8(8):CD006822. doi: 10.1002/14651858.CD006822.pub6. Cochrane Database Syst Rev. 2021. PMID: 34397099 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- Traub SJ, Wijdicks EF (2016) Initial diagnosis and management of coma. Emerg Med Clin N Am 34:777–793 - PubMed
-
- Posner JB, Plum F, Saper CB (2007) Plum and Posner’s diagnosis of stupor and coma. Oxford University Press, New York
-
- Volk S, Koedel U, Pfister HW, Schwankhart R, Op den Winkel M, Muhlbauer K, Klein M (2018) Impaired consciousness in the emergency department. Eur Neurol 80:179–186 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
