

The sodium-glutamate antagonist riluzole improves outcome after acute spinal cord injury: results from the RISCIS randomised controlled trial analysed using a global statistical analytic technique
- PMID: 40712181
- PMCID: PMC12309938
- DOI: 10.1016/j.ebiom.2025.105863
The sodium-glutamate antagonist riluzole improves outcome after acute spinal cord injury: results from the RISCIS randomised controlled trial analysed using a global statistical analytic technique
Abstract
Background: Spinal cord injury (SCI) clinical trials typically rely on a single primary endpoint to assess drug efficacy. This strategy fails to adequately capture the full impact of treatment in heterogenous neurological conditions like SCI. A more patient-centric analysis requires assessment of neurological function, functional capacity, and quality of life, incorporating meaningful patient-reported outcomes. The global statistical test (GST) addresses this challenge using a unified statistical conclusion regarding the superiority of a treatment strategy over another by evaluating multiple trial endpoints simultaneously.
Methods: The RISCIS trial (Safety and Efficacy of Riluzole in Acute Spinal Cord Injury Study) data was analysed using a multivariate nonparametric GST, integrating the total American Spinal Injury Association (ASIA) motor score (TOTM), Spinal Cord Independence Measure (SCIM), and SF-36 PCS (Short Form-36 Physical Component Scale) scores. In the RISCIS trial, patients with severe cervical SCI (AIS A, B, and C) were randomised to receive riluzole or placebo within 12 h of injury in a double blinded fashion. We compared six-month outcomes between groups using a modified O'Brien's rank sum test with sample variance adjustment. Higher summed ranks represent better global outcomes. The overall probability of improvement was computed using a summary estimate, the global treatment effect (GTE).
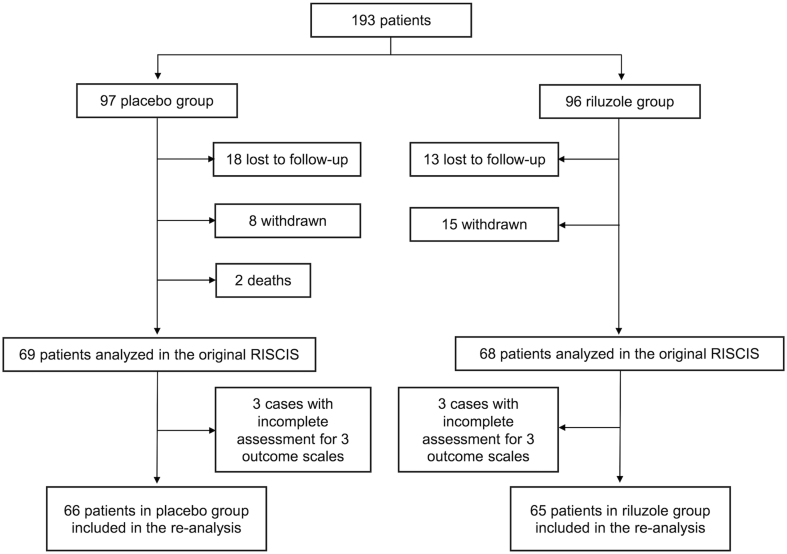
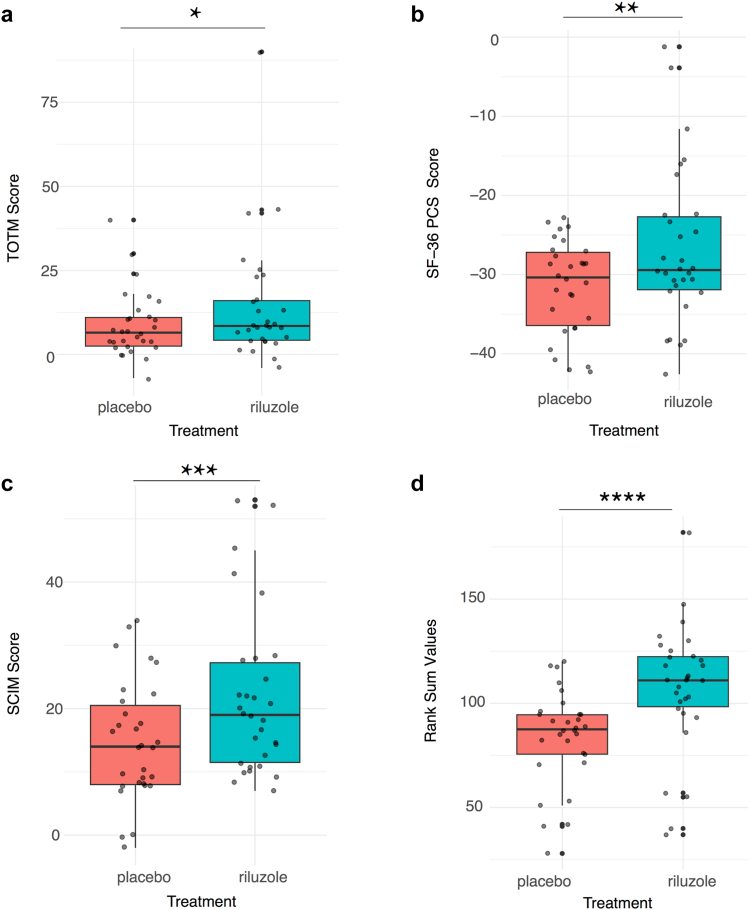
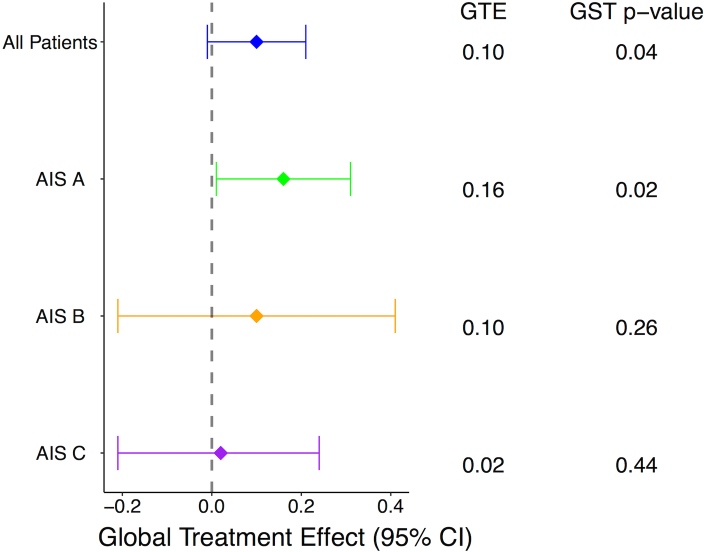
Findings: A total of 131 patients (mean age 45.8 years old, 82% males) completed the six-month outcome assessment. Among these, 49.6% were classified as AIS A, 20.6% as AIS B, and 29% as AIS C. Riluzole was administered within 12 h from injury for 14 days in 65 patients, while 66 received a placebo. The unadjusted mean change from baseline to six months showed a favourable response in the riluzole group compared to placebo across TOTM (p = 0.28 by t-test; p = 0.26 by Wilcoxon test), SCIM (p = 0.04 by t-test; p = 0.02 by Wilcoxon test), or SF-36 PCS (p = 0.23 by t-test; p = 0.21 by Wilcoxon test) scores. Using the GST to simultaneously assess these measures, the riluzole group exhibited a higher rank sum compared to placebo [median rank sum = 207 (IQR: 166-246) in riluzole vs 185 (IQR: 146-236) in placebo, p = 0.04]. Subgroup analysis revealed the greatest treatment benefit among patients with AIS A injuries (GTE = 0.16, 95% CI: 0.01-0.31, p = 0.02). At six months, the probability that riluzole treatment resulted in overall better outcomes than placebo across all assessed outcomes was 58%.
Interpretation: Riluzole was associated with improved global outcomes in patients with severe traumatic SCI, based on a composite score integrating ASIA total motor scores, SCIM, and SF36 outcomes at six months. Riluzole is a promising therapeutic option in SCI, but further investigation through higher-quality studies incorporating multidimensional assessments is warranted.
Funding: No funding was received for the present work. The original clinical trial (NCT01597518) was funded by the AO Foundation, United States Department of Defense (DOD), and the Praxis Spinal Cord Institute.
Keywords: Clinical trial; Global statistical test; Neuroprotection; Riluzole; Spinal cord injury.
Copyright © 2025 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests The authors have no relevant conflicts to disclose. WZR discloses consulting for Globus, Depuy, Seaspine, Acera, Expanding Innovations, outside of the submitted work. FUA discloses relationships with Stryker Spine, outside of the submitted work. JDG discloses being Co-Chair of the North American Clinical Trials Network, outside of the submitted work. JRW discloses relationships with Canadian Institutes of Health Research, Stryker Canada, Neuraxis, Canadian Medical Protective Agency, and Medcura, outside of the submitted work. AN discloses relationships with AO Spine North America, Premia Spine, Allosource, Depuy, and 3 Spine, outside of the submitted work.
Figures
Similar articles
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2020 Jan 9;1(1):CD011535. doi: 10.1002/14651858.CD011535.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 19;4:CD011535. doi: 10.1002/14651858.CD011535.pub4. PMID: 31917873 Free PMC article. Updated.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
