

Modification of the Association of B-Type Natriuretic Peptides With Mortality and Hospitalization Outcomes by Sex
- PMID: 40712268
- PMCID: PMC12311523
- DOI: 10.1016/j.jacadv.2025.101999
Modification of the Association of B-Type Natriuretic Peptides With Mortality and Hospitalization Outcomes by Sex
Abstract
Background: The effects of sex on the prognostic implications of natriuretic peptide (NP) elevation have not been fully elucidated in the population.
Objectives: The purpose of this study was to examine if sex modifies associations of NPs with mortality and hospitalization.
Methods: In a population-based retrospective cohort study, we identified all patients (aged ≥40 years) undergoing NP testing in Ontario, Canada (2015-2020). We examined for the presence of sex-by-NP interactions for 1-year outcomes and conducted sex-specific analyses for continuously increasing NP concentrations.
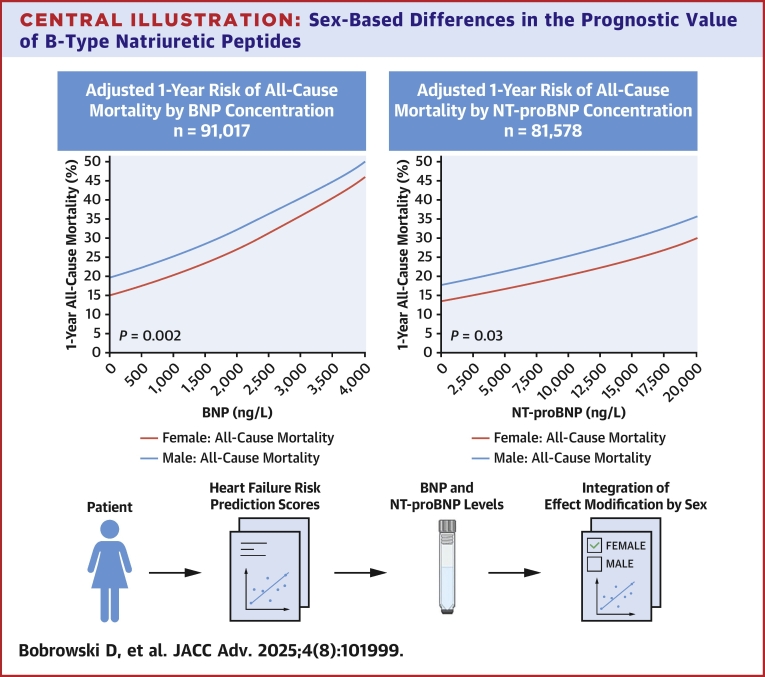
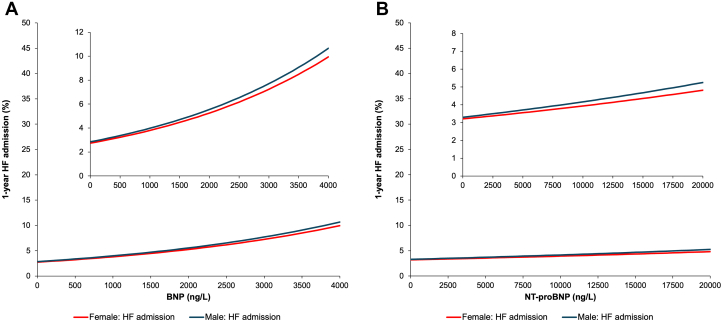
Results: We studied 91,017 individuals with B-type natriuretic peptide (BNP) tests (median 75 years; 48.0% females) and 81,578 individuals with N-terminal pro-BNP (NT-proBNP) tests (74 years; 48.6% females). Adjusted 1-year risks of all-cause mortality at any given NP concentration were higher in males than females. For example, 1-year mortality at a BNP of 400 ng/L was 16.8% in females and 21.6% in males. At an NT-proBNP of 900 ng/L, 1-year mortality was 14.2% in females and 18.5% in males. However, there were also significant sex interactions with BNP (P = 0.002) and NT-proBNP (P = 0.03) for mortality outcomes. When we examined cardiovascular hospitalizations, there was also a significant sex-by-NP interaction. For BNP, the risk of cardiovascular hospitalization was higher in males at lower concentrations but was higher in females at higher concentrations (P-interaction = 0.005). For NT-proBNP, the risk of cardiovascular hospitalization was higher in males at lower NP concentrations, but the gap narrowed at higher NP levels (P interaction = 0.03).
Conclusions: Sex modifies the association between NP concentrations and all-cause mortality or cardiovascular hospitalizations. Prognostically, interpretation of NP levels should consider effect modification by sex.
Keywords: B-type natriuretic peptide; heart failure; hospitalization; mortality; natriuretic peptides; sex.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding support and author disclosures This study was supported by a Foundation grant from the Canadian Institutes of Health Research (grant # FDN 148446) and also supported by the ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Dr Abdel-Qadir was supported by a National New Investigator Award from the Heart and Stroke Foundation of Canada and is currently supported by Tier 2 Canada Research Chair in Cardiovascular Disease Epidemiology and Outcomes. Dr McNaughton is supported by the Sunnybrook Research Institute, the Practice Plan of the Department of Emergency Services at Sunnybrook Health Sciences Centre and the University of Toronto. Dr Lee is the Ted Rogers Chair in Heart Function Outcomes, University Health Network, University of Toronto. Dr Doumouras is supported by the Women in Cardiology Fund from the Temerty Faculty of Medicine, University of Toronto. Dr Kavsak has received grants/reagents/consultant/advisor/honoraria from diagnostic companies that manufacture NP assays and materials for testing, including Abbott Laboratories, Abbott Point of Care, Beckman Coulter, Ortho Clinical Diagnostics, Quidel, Randox Laboratories, Roche Diagnostics, Siemens Healthcare Diagnostics, and Thermo Fisher Scientific. Dr Januzzi reports equity holdings in Imbria Pharma, Jana Care, and Fibrosys, current/recent grant support from Abbott, Applied Therapeutics, AstraZeneca, BMS, Novartis Pharmaceuticals, consulting income from Abbott Diagnostics, Beckman-Coulter, Jana Care, Janssen, Novartis, Prevencio, Quidel, and Roche Diagnostics, and serves on clinical endpoint committees/data safety monitoring boards for Abbott, AbbVie, Amgen, CVRx, Medtronic, Pfizer, and Roche Diagnostics. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




Similar articles
-
Brain natriuretic peptide and N-terminal brain natriuretic peptide for the diagnosis of haemodynamically significant patent ductus arteriosus in preterm neonates.Cochrane Database Syst Rev. 2022 Dec 8;12(12):CD013129. doi: 10.1002/14651858.CD013129.pub2. Cochrane Database Syst Rev. 2022. PMID: 36478359 Free PMC article.
-
The comparative and added prognostic value of biomarkers to the Revised Cardiac Risk Index for preoperative prediction of major adverse cardiac events and all-cause mortality in patients who undergo noncardiac surgery.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD013139. doi: 10.1002/14651858.CD013139.pub2. Cochrane Database Syst Rev. 2021. PMID: 34931303 Free PMC article.
-
Sex as a prognostic factor for mortality in adults with acute symptomatic pulmonary embolism.Cochrane Database Syst Rev. 2025 Mar 20;3(3):CD013835. doi: 10.1002/14651858.CD013835.pub2. Cochrane Database Syst Rev. 2025. PMID: 40110896
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
B-type natriuretic peptide-guided versus symptom-guided therapy in outpatients with chronic heart failure: a systematic review with meta-analysis.J Cardiovasc Med (Hagerstown). 2014 Feb;15(2):122-34. doi: 10.2459/JCM.0b013e328364bde1. J Cardiovasc Med (Hagerstown). 2014. PMID: 24522083
References
-
- Heidenreich P.A., Bozkurt B., Aguilar D., et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. J Am Coll Cardiol. 2022;79(17):1757–1780. doi: 10.1016/j.jacc.2021.12.011. - DOI - PubMed
-
- Ponikowski P., Voors A.A., Anker S.D., et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18(8):891–975. doi: 10.1002/ejhf.592. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
