

Coronary Artery Disease-Based Polygenic Risk Score in Early-Onset Acute Myocardial Infarction Subtypes
- PMID: 40712269
- PMCID: PMC12311502
- DOI: 10.1016/j.jacadv.2025.101994
Coronary Artery Disease-Based Polygenic Risk Score in Early-Onset Acute Myocardial Infarction Subtypes
Abstract
Background: The coronary artery disease-based polygenic risk score (PRS-CAD) estimates risk of acute myocardial infarction (AMI), but its performance across AMI subtypes in younger individuals, especially women, remains uncertain.
Objectives: The authors assessed PRS-CAD's performance in AMI subtypes.
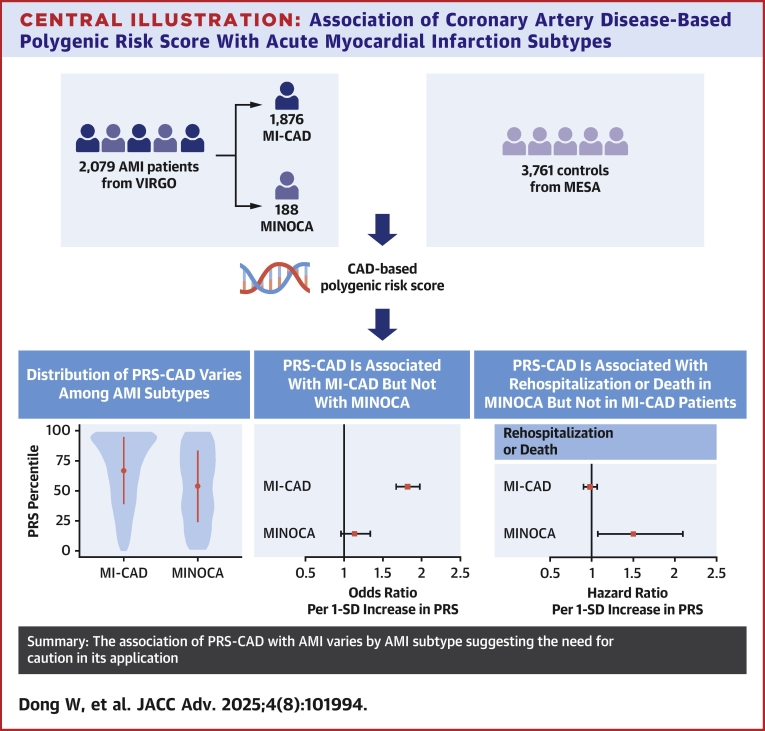
Methods: We included 2,079 AMI patients aged 18 to 55 years with a 2:1 female-to-male ratio from the VIRGO (Variation in Recovery: Role of Gender on Outcomes of Young Acute Myocardial Infarction Patients) study and 3,761 controls from the MESA (Multi-Ethnic Study of Atherosclerosis) study. AMI subtypes were classified using the VIRGO taxonomy. We evaluated PRS-CAD's association with AMI subtypes using multinomial logistic regression and with 1-year outcomes in AMI subtypes using Cox regression.
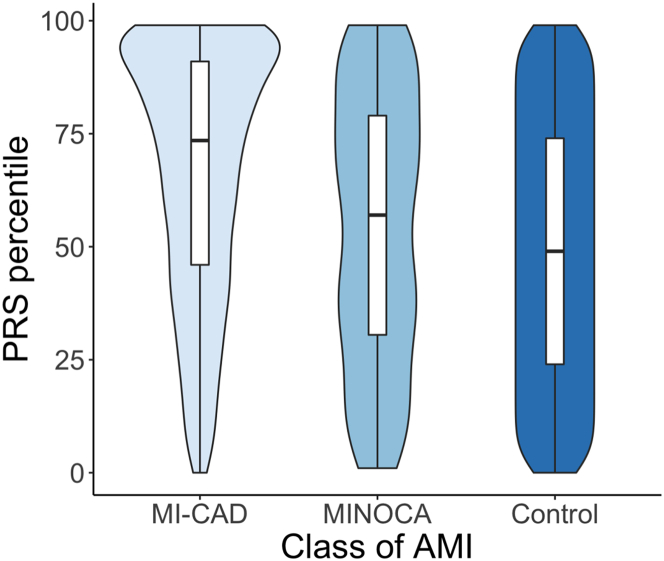
Results: PRS-CAD was significantly associated with MI due to coronary artery disease (N = 1,876; OR: 1.82 per 1-SD increase; 95% CI: 1.67-1.97; P < 0.001) but not with MI with nonobstructive coronary artery disease (N = 188; OR: 1.13 per 1-SD increase; 95% CI: 0.96-1.34; P = 0.14). PRS-CAD's performance did not differ by sex. A 1-SD increase in PRS-CAD was associated with higher risk of 1-year hospitalization or death in patients with MI with nonobstructive coronary artery disease (HR: 1.50; 95% CI: 1.08-2.10; P = 0.02) but not in patients with MI due to coronary artery disease (HR: 0.98; 95% CI: 0.91-1.07; P = 0.67).
Conclusions: PRS-CAD's association with AMI varied by subtype but not by sex in young adults, warranting caution in application.
Keywords: acute myocardial infarction; polygenic risk score; subtypes.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding support and author disclosures The VIRGO study was supported by grant R01 HL081153 from the National Heart, Lung, and Blood Institute (NHLBI). Whole genome sequencing (WGS) for the Trans-Omics in Precision Medicine (TOPMed) program was supported by the NHLBI. WGS for “NHLBI TOPMed: Multi-Ethnic Study of Atherosclerosis (MESA)” (phs001416.v3.p1) was conducted at the Broad Institute of MIT and Harvard (3U54HG003067-13S1). Centralized read mapping and genotype calling, along with variant quality metrics and filtering, were provided by the TOPMed Informatics Research Center (3R01HL-117626-02S1). Phenotype harmonization, data management, sample identity quality control, and general study coordination were provided by the TOPMed Data Coordinating Center (3R01HL-120393-02S1) and TOPMed MESA Multi-Omics (HHSN2682015000031/HSN26800004). The MESA projects are conducted and supported by the NHLBI in collaboration with MESA investigators. Funding support for MESA is provided by contracts 75N92020D00001, HHSN268201500003I, N01-HC-95159, 75N92020D00005, N01-HC-95160, 75N92020D00002, N01-HC-95161, 75N92020D00003, N01-HC-95162, 75N92020D00006, N01-HC-95163, 75N92020D00004, N01-HC-95164, 75N92020D00007, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168, N01-HC-95169, UL1-TR-000040, UL1-TR-001079, UL1-TR-001420, UL1TR001881, DK063491, R01HL105756, and R01HL146860. In the past 3 years, Dr Sawano has been partially supported by research funding from Polybio, Pfizer, and Novartis through Yale University; he has also received lecture honoraria from Boehringer Ingelheim. Dr Krumholz has received options for Element Science and Identifeye and payments from F-Prime for advisory roles; and he is a co-founder of and holds equity in Hugo Health, Refactor Health, and ENSIGHT-AI. He is associated with research contracts through Yale University from Janssen, Kenvue, Novartis, and Pfizer. Dr Lu has received support from the Sentara Research Foundation, the National Heart, Lung, and Blood Institute of the National Institutes of Health (under awards R01HL69954 and R01HL169171), and the Patient-Centered Outcomes Research Institute (under award HM-2022C2-28354) outside of the submitted work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



Similar articles
-
Appraisal of multiple polygenic risk scores to estimate the risk of myocardial infarction and coronary artery lesions.Commun Med (Lond). 2025 Jul 1;5(1):264. doi: 10.1038/s43856-025-00981-w. Commun Med (Lond). 2025. PMID: 40593158 Free PMC article.
-
The distinct subtypes and prognosis of acute myocardial infarction in antiphospholipid syndrome patients.Clin Rheumatol. 2025 Aug 18. doi: 10.1007/s10067-025-07624-4. Online ahead of print. Clin Rheumatol. 2025. PMID: 40824342
-
Exercise-based cardiac rehabilitation for coronary heart disease.Cochrane Database Syst Rev. 2016 Jan 5;2016(1):CD001800. doi: 10.1002/14651858.CD001800.pub3. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2021 Nov 6;11:CD001800. doi: 10.1002/14651858.CD001800.pub4. PMID: 26730878 Free PMC article. Updated.
-
Short-term exposure to ambient air pollution increased in-hospital non-ST-elevation myocardial infarction mortality risk, but not ST-elevation myocardial infarction: case-crossover based evidence from Beijing, China.Front Public Health. 2025 Jun 20;13:1613082. doi: 10.3389/fpubh.2025.1613082. eCollection 2025. Front Public Health. 2025. PMID: 40620562 Free PMC article.
-
Preoperative coronary interventions for preventing acute myocardial infarction in the perioperative period of major open vascular or endovascular surgery.Cochrane Database Syst Rev. 2024 Jul 3;7(7):CD014920. doi: 10.1002/14651858.CD014920.pub2. Cochrane Database Syst Rev. 2024. PMID: 38958136 Free PMC article.
References
-
- Manikpurage H.D., Eslami A., Perrot N., et al. Polygenic risk score for coronary artery disease improves the prediction of early-onset myocardial infarction and mortality in men. Circ Genom Precis Med. 2021;14(6) - PubMed
-
- Xu H., Hon C., Kaiser S., et al. Coronary artery disease polygenic risk score identifies patients at higher risk for recurrent cardiovascular events in the CANTOS trial. Circ Genom Precis Med. 2021;14(6) - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
