

The Secret Life of a Lost Guidewire
- PMID: 40713126
- PMCID: PMC12441537
- DOI: 10.1016/j.jaccas.2025.104181
The Secret Life of a Lost Guidewire
Abstract
Background: Lost guidewires during central venous catheterization are rare but serious, requiring prompt removal to reduce morbidity and mortality.
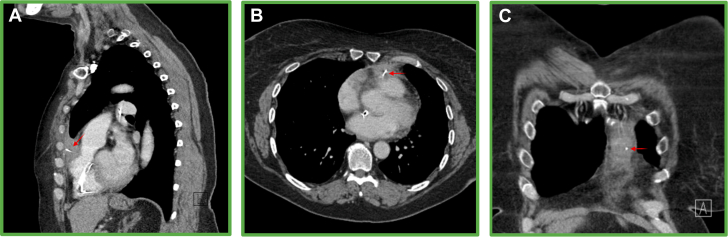
Case summary: A 58-year-old woman presented with a pulsating back mass and a spontaneous bruise under her left clavicle. More than 10 years ago, a 0.035-inch guidewire had been lost in her circulation, and retrieval attempts had failed. Computed tomography scan revealed a fragmented guidewire that had crossed into the arterial circulation through a patent foramen ovale and extended through the anterior mediastinum. After a discussion among the heart team, the decision was made to remove the wire percutaneously.
Discussion: This case highlights the risks of guidewire loss and the successful use of advanced catheter techniques for complex wire retrieval.
Take-home messages: Iatrogenic guidewire loss is associated with significant risk of morbidity and mortality, and the guidewire must be removed. A fragmented wire can be removed percutaneously by forming a free loop with an additional wire. If wire embolization is recognized during central venous catheter insertion, several bedside techniques can be attempted to rapidly correct the complication.
Keywords: CT; complication; guidewire; patent foramen ovale.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Samuel McGrath is undergoing a Clinical Research Training Fellowship (CRTF) funded by the British Heart Foundation (FS/CRTF/22/24187). Prof Hildick-Smith is a Proctor/Advisory to Abbott, Boston, Medtronic, and Edwards.
Figures






References
-
- National Institute for Clinical Excellence . 2002. Guidance on the use of ultrasound locating devices for placing central venous catheters.https://www.nice.org.uk/guidance/ta49/resources/guidance-on-the-use-of-u...
-
- Mariyaselvam M.Z.A., Patel V., Young H.E., Blunt M.C., Young P.J. Central venous catheter guidewire retention: lessons from England’s never event database. J Patient Saf. 2022;18:e387–e392. - PubMed
-
- Monaca E., Trojan S., Lynch J., Doehn M., Wappler F. Broken guide wire - a fault of design? Can J Anesth Can Anesth. 2005;52:801–804. - PubMed
-
- Fisher R., Ferreyro R. Evaluation of current techniques for nonsurgical removal of intravascular iatrogenic foreign bodies. Am J Roentgenol. 1978;130:541–548. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
