

Phase 1b/2 study evaluating safety, efficacy and immune effects of TLR9 agonist cavrotolimod with anti-PD-1 antibodies among patients with advanced solid tumors
- PMID: 40713179
- PMCID: PMC12306225
- DOI: 10.1136/jitc-2025-011651
Phase 1b/2 study evaluating safety, efficacy and immune effects of TLR9 agonist cavrotolimod with anti-PD-1 antibodies among patients with advanced solid tumors
Abstract
Background: There is an unmet need for novel immunotherapies to overcome immune evasion in patients with advanced skin cancers resistant to programmed death (PD)-1 / PD-ligand 1 (PD-L1) blockade. Cavrotolimod is a novel spherical nucleic acid configuration of a toll-like receptor 9 agonist oligonucleotide, designed to trigger innate and adaptive immune responses to tumors.
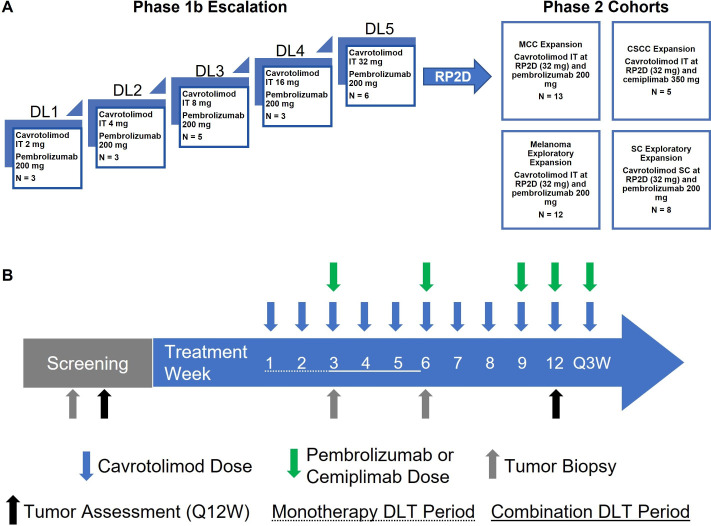
Patients and methods: The safety, pharmacokinetics, pharmacodynamics and preliminary efficacy of intratumoral cavrotolimod, first dosed alone and then in combination with anti-PD-1 antibodies (pembrolizumab or cemiplimab), were assessed in a combined Phase 1b/2 dose escalation/dose expansion study in patients with advanced skin cancers, including melanoma, Merkel cell carcinoma and cutaneous squamous cell carcinoma (www.
Clinicaltrials: gov; NCT03684785).
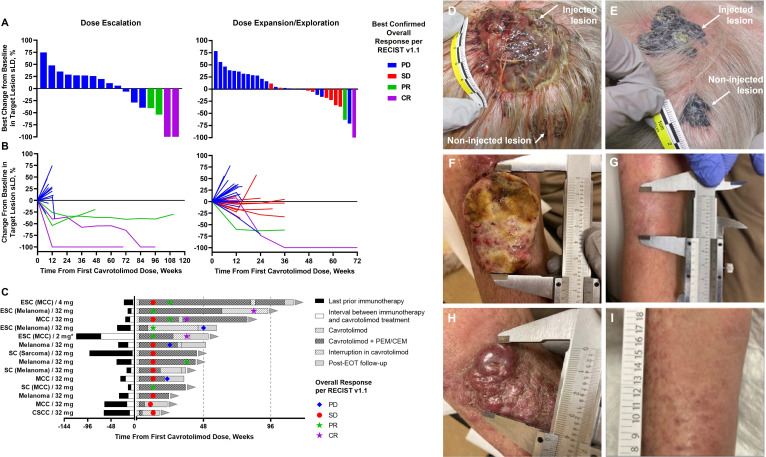
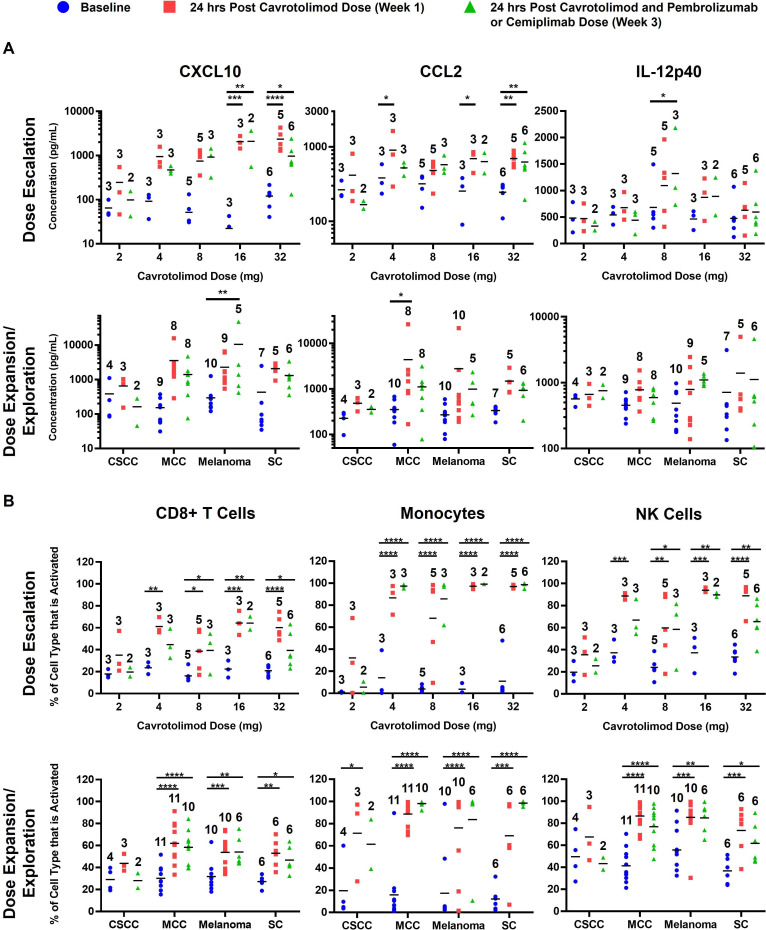
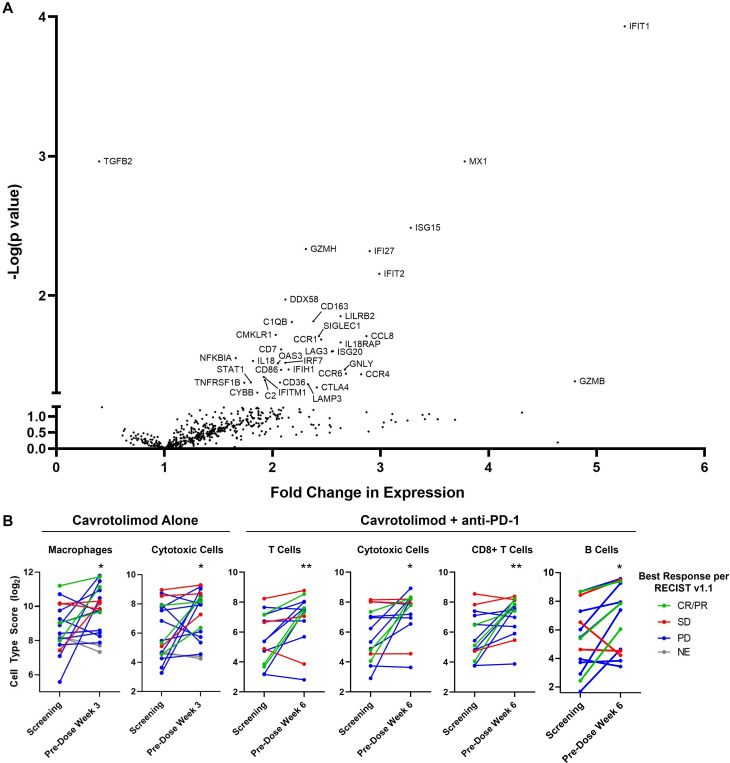
Results: A total of 58 patients (20 in dose-escalation and 38 in expansion cohorts) were enrolled. 55 (95%) of the 58 patients experienced progressive disease on prior anti-PD-(L)1 therapy. Cavrotolimod, in combination with anti-PD-1 therapy, produced objective responses in 6 (12%) and stable disease (SD) in 8 (16%) of 51 evaluable patients on this study, leading to a disease control rate of 27% (14/51). 5 of 6 (83%) patients with an objective response and 13 of 14 (93%) patients with disease control had progressed on prior anti-PD-(L)1 therapy. Disease control was durable, with median duration of 54 (range 24-88+) weeks for responses and 24 (range 11-35+) weeks for SD. Regression of both injected and non-injected tumors was observed. Cavrotolimod, alone and in combination with anti-PD-1 therapy, had a manageable safety profile with mostly transient adverse events (AEs). The most frequent Grade 3/4 cavrotolimod-related AEs were fatigue and injection site reactions. Cavrotolimod dosing was associated with robust chemokine/cytokine induction and lymphocyte activation in peripheral blood. Serial tumor biopsies of injected tumors suggested upregulation of genes associated with the interferon pathway, antiviral proteins, immune checkpoints, chemokines, granzymes and costimulatory proteins, along with increases in certain immune cell populations.
Conclusions: Cavrotolimod had a manageable safety profile and showed clinical activity in anti-PD-(L)1 refractory cutaneous malignancies, suggesting potential for further development as an antitumor immunotherapy in combination with other agents.
Trial registration number: NCT03684785.
Keywords: Immune Checkpoint Inhibitor; Intratumoral; Nanoparticle; Skin Cancer; Toll-like receptor - TLR.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: WD, DEF, SM and LS were employees of the study sponsor, Exicure Inc. GJH and SB report consulting or advisory board fees from the study sponsor. TMW-D, GJH, TM, AID, BAH and SB report consulting, advisory board membership or institutional research funding related to Merck. GJH, TM, AID and SB consulting, advisory board membership or institutional research funding related to Regeneron. WD and AB report patent filings related to the use of cavrotolimod in antitumor therapy.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials