

hCCL19-expressing recombinant Newcastle disease virus boosts CAR T cell infiltration and efficacy in solid tumor
- PMID: 40713180
- PMCID: PMC12306363
- DOI: 10.1136/jitc-2025-011783
hCCL19-expressing recombinant Newcastle disease virus boosts CAR T cell infiltration and efficacy in solid tumor
Abstract
Background: Chimeric antigen receptor (CAR) T cell therapy has revolutionized the treatment of hematological malignancies; however, it faces significant challenges in treating solid tumors, including limited immune infiltration into tumor tissues and immunosuppressive tumor microenvironment. Oncolytic viruses (OVs), which selectively destroy cancer cells and trigger antitumor immune responses, offer a compelling solution to these challenges. Newcastle disease virus (NDV) is a natural OV that exhibits antitumor activity with minimal side effects in clinical studies. We hypothesized that combining NDV, engineered to express a chemokine, with tetracycline-inducible CAR T cells could synergistically enhance CAR T cell therapy efficacy against solid tumors.
Methods: We constructed a recombinant NDV expressing human CCL19 (rNDV19) and evaluated its therapeutic efficacy alongside doxycycline-inducible CAR T cells in an orthotopic lung cancer mouse model. Tumor burden, immune cell infiltration, and mouse survival were analyzed.
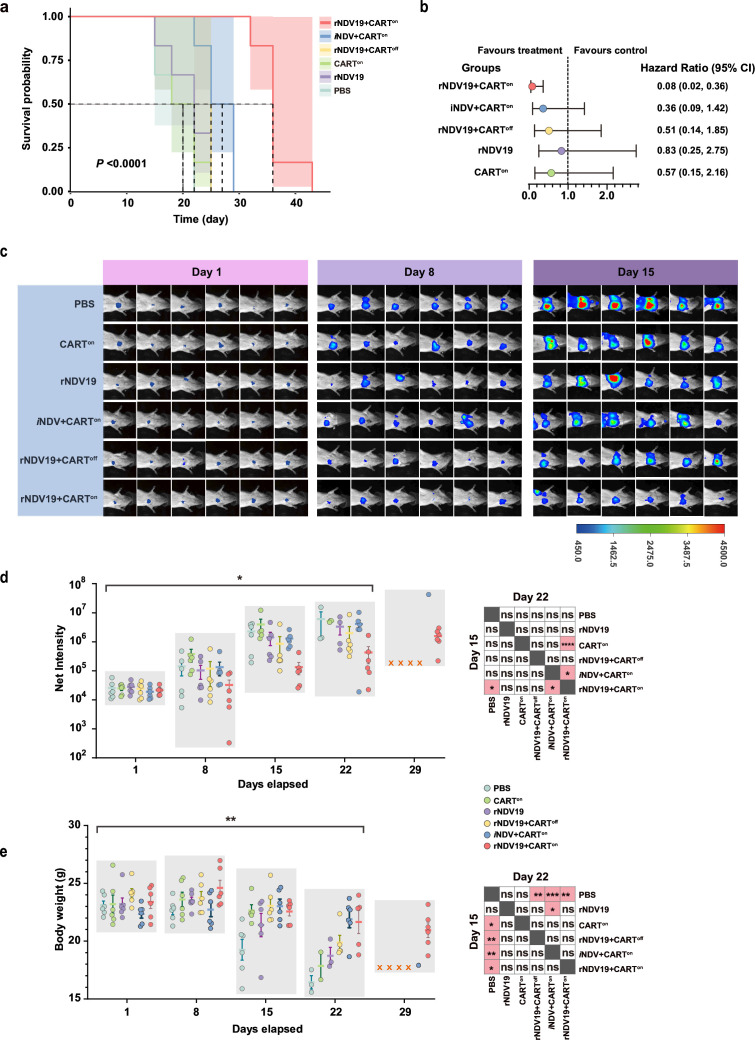
Results: rNDV19 retained potent oncolytic activity, significantly reducing tumor cell viability while achieving stable expression of human CCL19. rNDV19 triggered significant recruitment of CAR T cells into tumors and promoted their activity. Mechanistic analysis revealed that rNDV19 and CAR T cell combination therapy remodeled the tumor microenvironment. Transcriptomic profiling highlighted activation of critical immune pathways-including leukocyte chemotaxis, T cell differentiation, cytokine production, and immune response-activating signaling in combination therapy. These findings were further corroborated by upregulated expression of T cell activation markers like IL-2, TNF-α, IFN-γ, and cytotoxic effector molecules such as granzyme A and perforin. Therapeutically, the combination synergistically extended median survival time from 22 to 36 days, outperforming monotherapies.
Conclusions: The combination of rNDV19 and CAR T cells represents a promising strategy for overcoming the limitations of CAR T cell therapy for solid tumors. This approach enhances immune cell infiltration and activation, potentially converting "cold" tumors into "hot" tumors to improve therapeutic outcomes and offering a robust translational framework for solid tumor immunotherapy.
Keywords: Adoptive cell therapy - ACT; Oncolytic Viruses.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: No, there are no competing interests.
Figures





References
-
- FDA approves new car t-cell therapy for all. [15-Nov-2024]. https://www.aabb.org/news-resources/news/article/2024/11/12/fda-approves... Available. Accessed.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials