

Merkel Cell Carcinoma in Solid Organ Transplant Recipients: Prognosis and Response to Immunotherapy
- PMID: 40713931
- PMCID: PMC12597097
- DOI: 10.1093/bjd/ljaf304
Merkel Cell Carcinoma in Solid Organ Transplant Recipients: Prognosis and Response to Immunotherapy
Abstract
Background: Merkel cell carcinoma (MCC) is an aggressive skin cancer with an increased risk of occurrence in immunocompromised patients, including solid organ transplant recipients (SOTR). As the number of SOTR rises worldwide, MCC cases in this population are also expected to increase. While anti-programmed death-(ligand)1 (anti-PD-(L)1) immunotherapy generates durable tumor responses in ∼50% of immunocompetent (IC) patients with advanced MCC, its efficacy and safety in SOTR remain uncertain as these patients have been excluded from most clinical trials.
Objectives: To compare baseline characteristics and outcomes among SOTR and IC patients with MCC, and to evaluate efficacy and toxicity of anti-PD-(L)1 in SOTR.
Methods: We queried a MCC registry from our institution (April 1988-May 2024), extracting data on demographics, anti-PD-(L)1 response, immunosuppression regimens, and incidence of allograft rejection and failure for analysis.
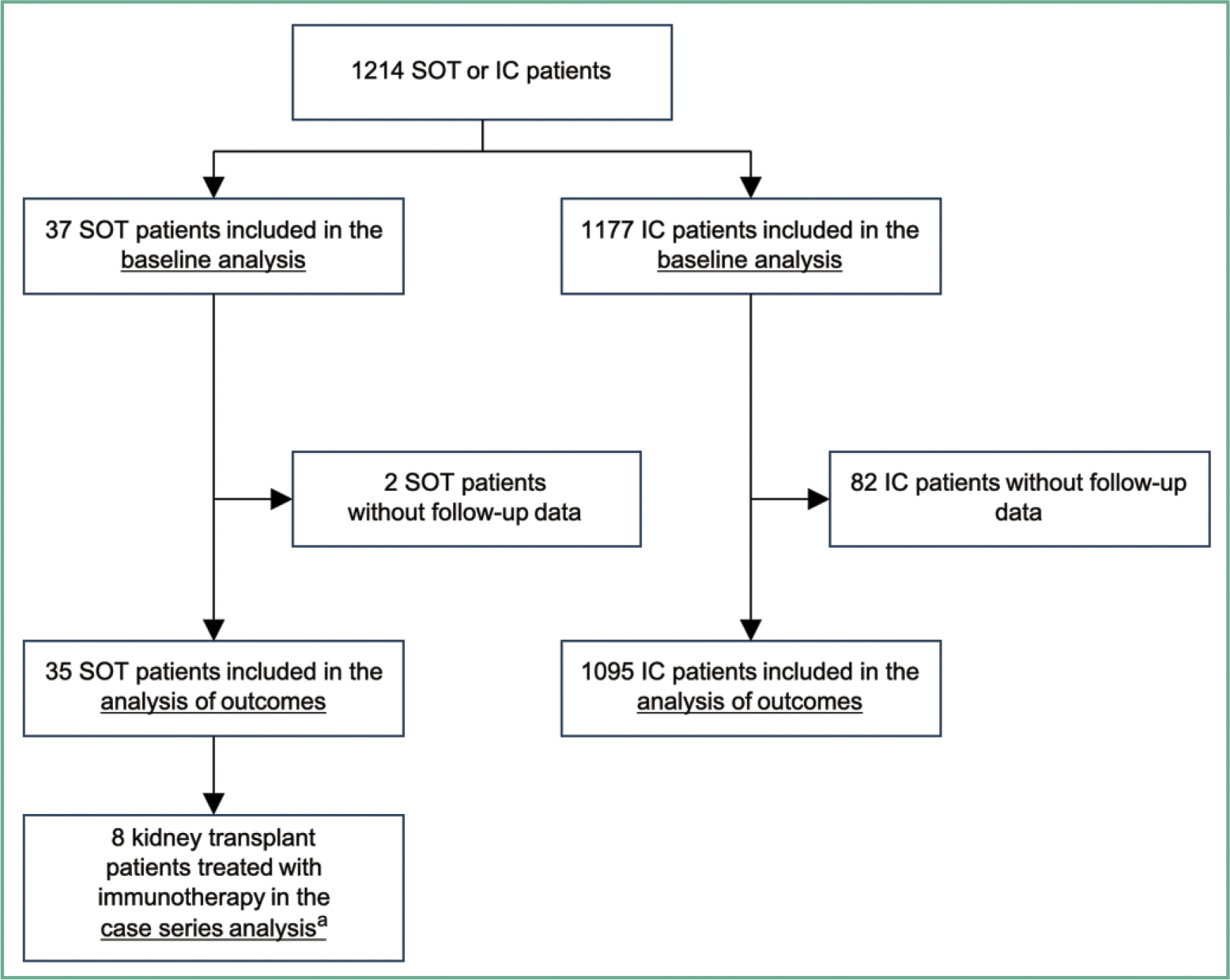
Results: We identified 1214 MCC patients (37 SOTR and 1177 IC patients); 8 of 37 SOTR received anti-PD-(L)1. The median time from solid organ transplant to MCC diagnosis was 10 years (range 0.4-43). The proportion of patients with advanced MCC (≥ stage III) was 76% in SOTR compared to 51% in IC patients (p=0.004). SOTR status was associated with worse outcomes, including higher rates of disease progression (adjusted hazard ratio [aHR] 2.3), MCC-specific mortality (aHR 3.0), and overall mortality (aHR 3.9; all p<0.001). The median time to death due to MCC for SOTR was 2.7 years; 24% of SOTR died within one year of diagnosis, in contrast to just 4% of IC patients. The median time to MCC progression for SOTR was 8.6 months vs 12 years for IC patients. Among SOTR, 70% developed distant metastases within 2 years versus 25% of IC patients. All eight MCC SOTR treated with anti-PD-(L)1 were kidney transplant recipients, with 5 (63%) experiencing an objective response (CR: 2, PR: 3). However, 2 (29%) patients experienced irreversible graft failure within 9 weeks.
Conclusions: SOTR status is a significant independent risk factor of a worse prognosis for MCC. This study represents the largest cohort evaluating the efficacy and safety of anti-PD-(L)1 in SOTR with advanced MCC, highlighting the potential benefits in this population.
© The Author(s) 2025. Published by Oxford University Press on behalf of British Association of Dermatologists. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
Conflicts of interest
D.S.H. has received research funding through his institution from the Kuni Foundation and GE HealthCare. E.H. has received research funding (institution) from AstraZeneca, Bristol Myers Squibb, Cullinan Oncology, Gilead Sciences, ImCheck Therapeutics, Immunocore, Kezar Life Sciences, NiKang Therapeutics, Neoleukin Therapeutics, Pfizer and Replimune; and he has received consulting fees from Eisai Co. S.B. has received consulting or advisory role fees and honoraria from Bristol Myers Squibb, Incyte and Replimune; and has received research funding from Agenus, Amphivena Therapeutics, Bristol Myers Squibb, Checkmate Pharmaceuticals/Regeneron, EMD Serono, Exicure, Incyte, Merck, 4SC, Seven and Eight Pharmaceuticals, TriSalus Life Sciences and Xencor. E.J.L. has served as a consultant/advisor for Agenus, Bristol Myers Squibb, CareDx, Eisai, Genentech, HUYA Bioscience International, Immunocore, Instil Bio, IO Biotech, Lyvgen Biopharma, Merck, Merck KGaA, Natera, Nektar, Novartis, OncoSec, Pfizer, Rain Therapeutics, Regeneron, Replimune, Sanofi-Aventis, Sun Pharma and Syneos Health; he has received institutional research funding from 1104Health, Bristol Myers Squibb, Haystack Oncology, Merck, Regeneron and Sanofi; and owns stock in Iovance (less than $10 K). C.D.B. has served as a consultant for Pierre Fabre; his institution has received research funding from the Kuni Foundation. P.N. has served as a consultant for EMD Serono, Merck and Sanofi/Regeneron; his institution has received research funding from Bristol Myers Squibb and EMD Serono. The remaining authors declare no conflicts of interest.
Figures


References
-
- Engels EA, Frisch M, Goedert JJ et al. Merkel cell carcinoma and HIV infection. Lancet 2002; 359:497–8. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
