

Clinical and molecular epidemiology of chikungunya outbreaks during 2019-2022 in India
- PMID: 40715163
- PMCID: PMC12297696
- DOI: 10.1038/s41598-025-09771-9
Clinical and molecular epidemiology of chikungunya outbreaks during 2019-2022 in India
Abstract
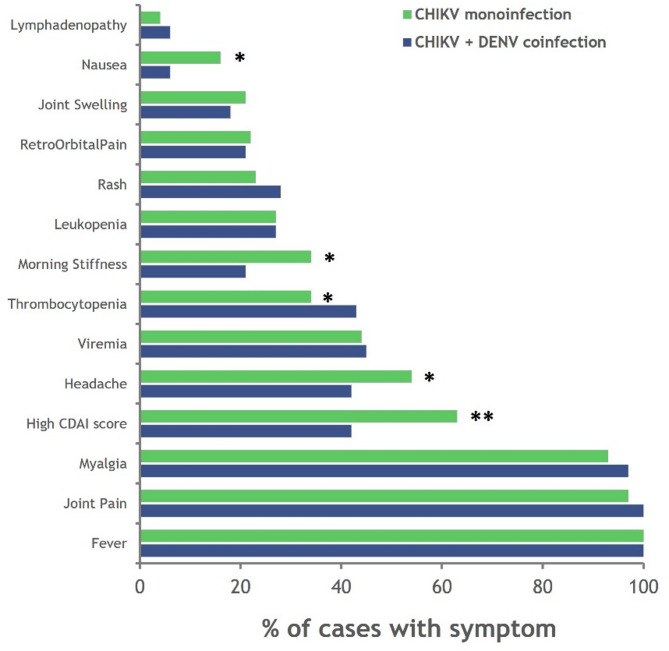
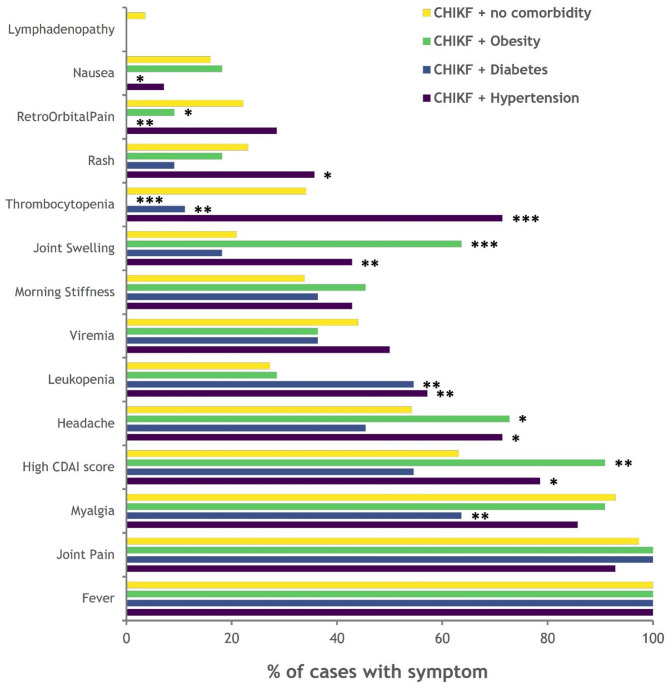
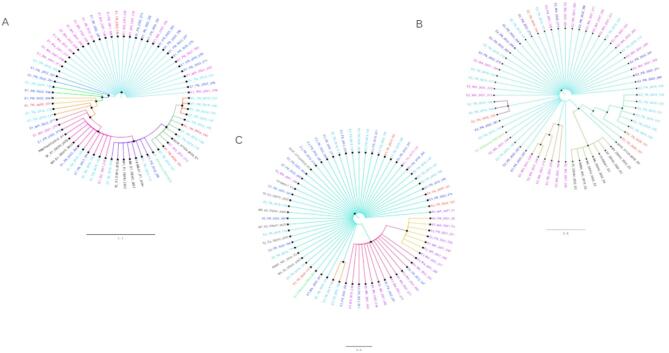
Chikungunya fever (CHIKF) is endemic in India, with multiple outbreaks occurring across the country since its reemergence in 2005. Suspected CHIKF patients were recruited from four clinical sites during 2019-2022, with data collected on sociodemographic, clinical, and epidemiological aspects. Sera samples were screened for IgM, IgG antibodies and viral RNA along with their neutralizing capacity. Envelope genes of Chikungunya virus (CHIKV) isolated were sequenced and further analysed. A total of 1312 suspected patients were screened during the study period; 258 patients were laboratory-confirmed with CHIKV infection. Severe clinical manifestation was observed in the patients during the viremic phase of infection. The neutralization potential was found to be increasing proportionally with the onset of illness, coinciding with the rise of IgG antibodies. Three of the four clinical sites had reported CHIKF outbreaks at different time points during the study period, and a distinct pattern of clinical presentation was observed across the sites. Phylogenetic and network analyses of E1, E2 and E3 genes from 62 CHIKV isolates demonstrated their evolution within the country. This study provides preliminary evidence of spatial and temporal variation in the clinical presentation and molecular evolution of virus in CHIKF outbreaks across India.
Keywords: CHIKV outbreaks; Chikungunya fever; Clinical epidemiology; Comorbidities; Dengue coinfection; Good health and well being; Molecular epidemiology; Spatial variation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures



References
-
- Facts about Chikungunya. Directorate of national vector borne disease control program. Ministry of Health and Family Welfare, Govt. of India. p. 6. https://nvbdcp.gov.in/WriteReadData/l892s/Facts_about_Chikungunya17806.pdf
-
- Suhrbier, A. Rheumatic manifestations of chikungunya: emerging concepts and interventions. Nat. Rev. Rheumatol.15 (10), 597–611. 10.1038/s41584-019-0276-9 (2019). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
