

A randomized controlled trial comparing large-volume band ligator and cyanoacrylate injection in the endoscopic management of actively bleeding gastric varices
- PMID: 40715299
- PMCID: PMC12297341
- DOI: 10.1038/s41598-025-12600-8
A randomized controlled trial comparing large-volume band ligator and cyanoacrylate injection in the endoscopic management of actively bleeding gastric varices
Abstract
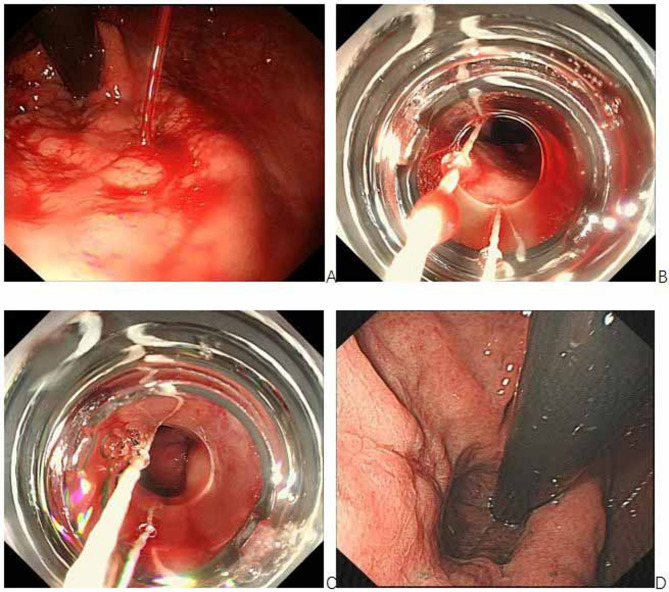
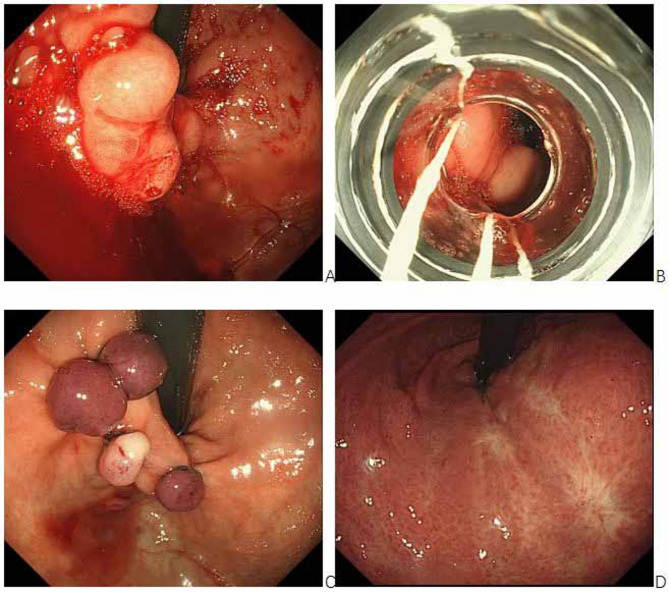
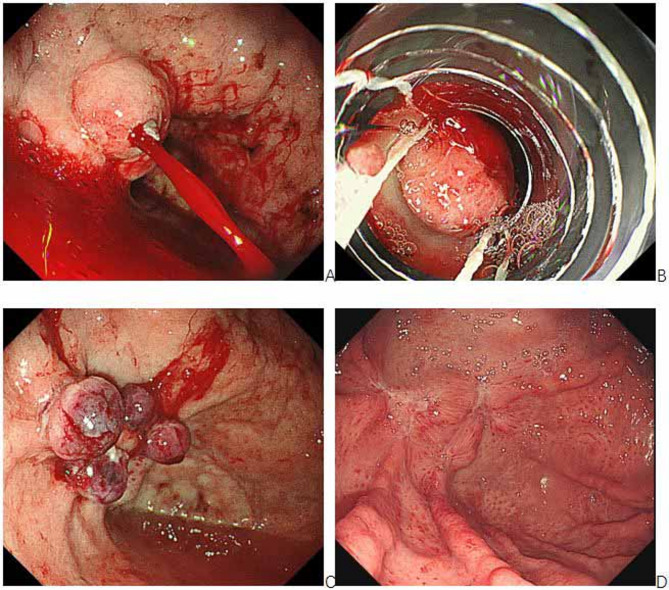
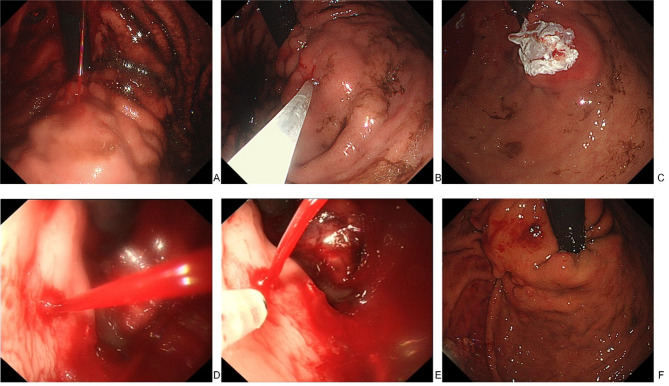
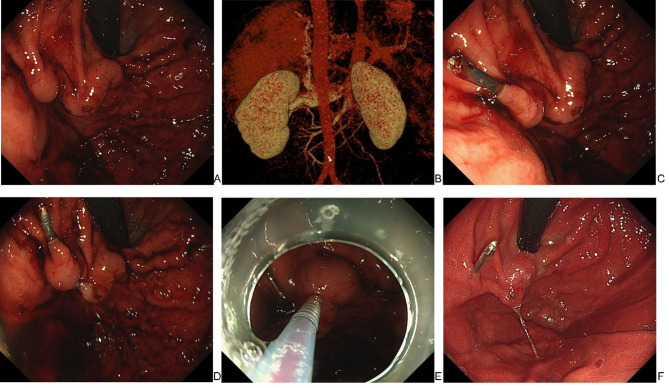
Managing actively bleeding gastric varices (GV) is clinically challenging. This study assessed the safety and efficacy of endoscopic band ligation (EBL) using large-volume ligators compared with endoscopic variceal obturation (EVO) in managing actively bleeding GV. Patients who were diagnosed with active GV bleeding via endoscopy and underwent EBL with large-volume band ligators or EVO were enrolled. Follow-up endoscopy was performed at 1, 3, and 6 months after endoscopic treatment. Primary outcomes were the initial haemostasis success rate, GV eradication rate within 3 months, 1-week rebleeding rate, 6-month cumulative rebleeding rate, and recurrence rate within 6 months. Secondary outcomes were the rate and average volume of blood transfusions in patients with rebleeding and adverse events related to endoscopic treatment. Overall, 154 patients were included (EBL group: n = 77; EVO group: n = 77). There were no statistically significant differences between the two groups regarding the initial haemostasis success rate, 1-week rebleeding rate, 3-month GV eradication rate and average number of sessions to GV eradication, cumulative rebleeding rate, and recurrence rate within 6 months. Three of the nine patients with rebleeding in the EVO group required blood transfusion with an average blood transfusion volume that was significantly lower than that required by the five patients with rebleeding in the EBL group (P = 0.024). The fever rate was lower in the EBL group than in the EVO group (P = 0.011). In the EVO group, one patient developed a pulmonary embolism and died during treatment, and three patients developed postoperative sepsis. The short-term efficacy of EBL with large-volume ligators in the treatment of actively bleeding GV is similar to that of EVO; however, postoperative rebleeding is often more dangerous in EBL than in EVO. Therefore, EBL represents a viable alternative in emergency endoscopic control of GV bleeding, provided that a contingency plan for early band slippage-related rebleeding is implemented.Trial registration: Chinese Clinical Trial Registry (No. ChiCTR1900027588, 19/11/2019).
Keywords: Endoscopic band ligation; Endoscopic injection; Gastric varices; Haemostasis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Endoscopic injection of cyanoacrylate glue versus other endoscopic procedures for acute bleeding gastric varices in people with portal hypertension.Cochrane Database Syst Rev. 2015 May 12;2015(5):CD010180. doi: 10.1002/14651858.CD010180.pub2. Cochrane Database Syst Rev. 2015. PMID: 25966446 Free PMC article.
-
Secondary prevention of variceal bleeding in adults with previous oesophageal variceal bleeding due to decompensated liver cirrhosis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Mar 30;3(3):CD013122. doi: 10.1002/14651858.CD013122.pub2. Cochrane Database Syst Rev. 2021. PMID: 33784794 Free PMC article.
-
Treatment for bleeding oesophageal varices in people with decompensated liver cirrhosis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 10;4(4):CD013155. doi: 10.1002/14651858.CD013155.pub2. Cochrane Database Syst Rev. 2021. PMID: 33837526 Free PMC article.
-
Combining endoscopic variceal ligation and omeprazole sodium in treating upper gastrointestinal hemorrhage combined with liver cirrhosis.BMC Gastroenterol. 2025 Jul 1;25(1):446. doi: 10.1186/s12876-025-04037-0. BMC Gastroenterol. 2025. PMID: 40596836 Free PMC article.
-
Comparing large-volume band ligators and cyanoacrylate injection for gastric variceal eradication: A prospective study.Medicine (Baltimore). 2022 Nov 18;101(46):e31939. doi: 10.1097/MD.0000000000031939. Medicine (Baltimore). 2022. PMID: 36401384 Free PMC article. Clinical Trial.
References
-
- Northup, P. G. & Caldwell, S. H. Treatment of bleeding gastric varices. J. Gastroenterol. Hepatol.20(11), 1631–1633. 10.1111/j.1440-1746.2005.04042.x (2005). - PubMed
-
- D’Amico G, De Franchis R, Cooperative Study Group. Upper digestive bleeding in cirrhosis. Post-therapeutic outcome and prognostic indicators. Hepatology38(3), 599–612. 10.1053/jhep.2003.50385 (2003). - PubMed
-
- Rao, A. S. et al. Combined endoscopic-interventional radiologic approach for the treatment of bleeding gastric varices in the setting of a large splenorenal shunt. Gastrointest Endosc.76(5), 1064–1065. 10.1016/j.gie.2011.10.013 (2012). - PubMed
-
- Hwang, J. H. et al. The role of endoscopy in the management of variceal hemorrhage. Gastrointest Endosc.80(2), 221–227. 10.1016/j.gie.2013.07.023 (2014). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
