

Do mini-fragment T-plates allow for more proximal rafting than pre-contoured anatomic plates in lateral split-depression tibial plateau fractures?
- PMID: 40715838
- PMCID: PMC12296757
- DOI: 10.1007/s00590-025-04435-w
Do mini-fragment T-plates allow for more proximal rafting than pre-contoured anatomic plates in lateral split-depression tibial plateau fractures?
Abstract
Purpose: To compare the proximity of rafting screws to the articular surface in lateral split-depression (LSD) tibial plateau fractures using mini-fragment (MF) and pre-contoured anterolateral (AL) proximal tibia plates. Secondary aims included comparing patient-reported outcome scores and rates of hardware failure and reoperation.
Methods: Design Retrospective review.
Setting: Multi-center Level I Tertiary Academic Center. Patient Selection Criteria: Adult patients with AO/OTA 41B3.1 LSD tibial plateau fractures treated over 30 months by a single surgeon were identified. Patients were included when their fractures were treated with either a MF T-plate (2.7 mm in thickness) or a pre-contoured anatomic AL plate.
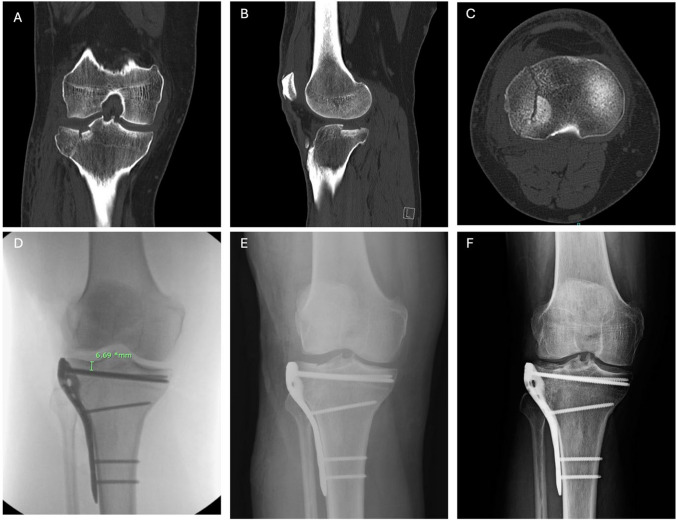
Main outcome measures: The primary outcome was the distance from the lateral joint line to the most proximal screw (screw-to-joint distance [SJD]) as measured on intraoperative fluoroscopy.
Results: Twenty-four patients were included with patients having received either a 2.7-mm MF T-plate (n = 14) or a standard AL proximal tibia plate (n = 10) and were followed for a median time of 29 weeks. Average SJD was 3.79 mm in the MF group and 8.67 mm in the AL group (p < 0.001). There was no difference in PROMIS scores between the groups. No patients experienced loss of reduction, implant loosening/failure, reoperation, or removal of tibial plateau hardware.
Conclusions: Mini-fragment plates allow for a significantly shorter SJD compared to AL plates, allowing surgeons to provide more proximal rafting of LSD fractures while maintaining low rates of postoperative complications. No increase in fracture subsidence was observed when using mini-fragment fixation alone compared to AL plates.
Keywords: Anterolateral plate; Fracture; Mini-fragment plate; Screw joint distance; Split-depression; Tibial plateau.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: Elizabeth Lechtholz-Zey: None. Michael Allen: None. Ivan Luu: None Ian Hasegawa: None Joseph T Patterson: AOTrauma North America: Board or committee member, research support; Bodycad: IP royalties, paid consultant; European Journal of Orthopaedic Surgery and Traumatology: Editorial or governing board; Globus Medical: Paid consultant; Johnson & Johnson: Paid consultant; Journal of Orthopaedic Trauma: Editorial or governing board; Orthopaedic Trauma Association: Board or committee member, research support; Stryker: Paid consultant Joshua L Gary: Stryker: Consulting and royalties; Smith and Nephew: Consulting and royalties; Curvafix: Consulting and stock options; SMV Scientific: Stockholder; Agnovos: Clinical Evaluation Committee Member “Restore” study; AO: Honoraria for teaching.
Figures

References
-
- Elsoe R, Larsen P, Nielsen NP, Swenne J, Rasmussen S, Ostgaard SE (2015) Population-based epidemiology of tibial plateau fractures. Orthopedics 38:e780-786. 10.3928/01477447-20150902-55 - PubMed
-
- Mthethwa J, Chikate A (2018) A review of the management of tibial plateau fractures. Musculoskelet Surg 102:119–127. 10.1007/s12306-017-0514-8 - PubMed
-
- Cho JW, Samal P, Jeon YS, Oh CW, Oh JK (2016) Rim plating of posterolateral fracture fragments (PLFs) through a modified anterolateral approach in tibial plateau fractures. J Orthop Trauma 30:362. 10.1097/BOT.0000000000000638 - PubMed
-
- Ye X, Huang D, Perriman DM, Smith PN (2019) Influence of screw to joint distance on articular subsidence in tibial-plateau fractures. ANZ J Surg 89:320–324. 10.1111/ans.14978 - PubMed
-
- Trenholm A, Landry S, McLaughlin K, Deluzio KJ, Leighton J, Trask K et al (2005) Comparative fixation of tibial plateau fractures using alpha-BSM, a calcium phosphate cement, versus cancellous bone graft. J Orthop Trauma 19:698–702. 10.1097/01.bot.0000183455.01491.bb - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
