

Identifying low-risk breast cancer patients for axillary biopsy exemption: a multimodal preoperative predictive model
- PMID: 40717102
- PMCID: PMC12302562
- DOI: 10.1186/s40001-025-02950-4
Identifying low-risk breast cancer patients for axillary biopsy exemption: a multimodal preoperative predictive model
Abstract
Background: As the most prevalent female malignancy worldwide, breast cancer frequently involves axillary lymph node metastasis (ALNM), which critically affects therapeutic algorithms. Current guidelines mandate preoperative ultrasound-guided axillary biopsy for suspicious lymph nodes, potentially exposing some low-risk patients with negative results to invasive risks. To optimize the utilization of biopsy, this study established a multimodal predictive framework that preoperatively assesses axillary lymph node (ALN) status, thereby triaging candidates for ultrasound-guided axillary biopsy.
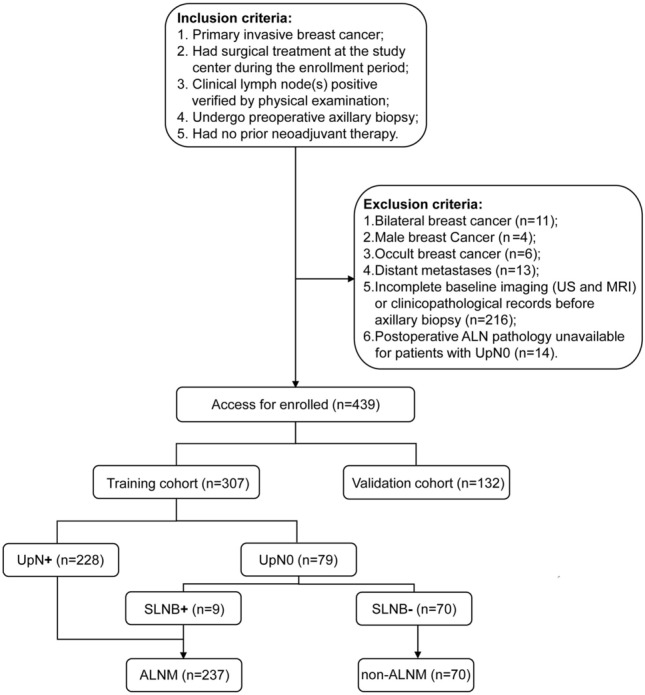
Methods: We conducted a retrospective single-center analysis of 703 breast cancer patients who underwent ultrasound-guided axillary biopsy with subsequent definitive surgery at the First Affiliated Hospital of Xi'an Jiaotong University (07/2020-05/2023). Following rigorous application of the inclusion/exclusion criteria, 439 eligible patients were randomized into training (n = 307, 69.9%) and validation (n = 132, 30.1%) cohorts. Axillary surgical pathology served as the reference standard for categorizing lymph node status. Multivariable predictors identified through the least absolute shrinkage and selection operator (LASSO) and logistic regression informed the construction of a clinically deployable nomogram. Model discrimination was quantified via receiver operating characteristic (ROC) analysis with area under the curve (AUC) calculations. The optimal threshold was determined using the maximum Youden index.
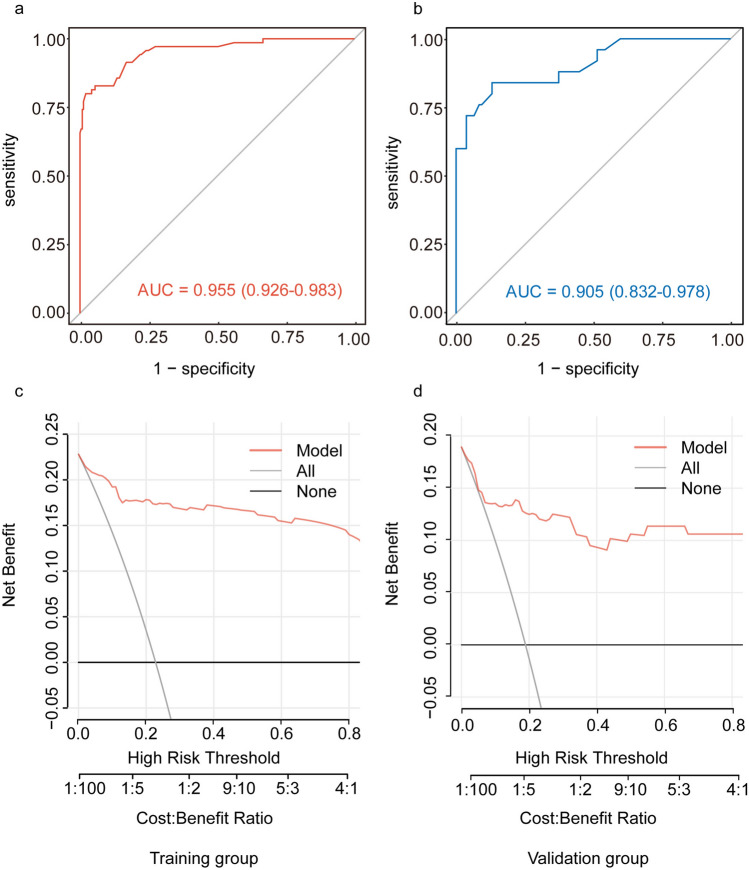
Results: LASSO, univariate, and multivariate logistic regression analyses revealed that estrogen receptor (ER) status (P = 0.007), ALN cortical-medullary boundary (P = 0.012), ALN cortical thickness (P < 0.001), short-axis diameter (P = 0.032), and the BI-RADS category on magnetic resonance imaging (MRI) (P = 0.021) were independent predictors of non-ALNM. A nomogram was constructed based on these factors. The multimodal model demonstrated excellent discrimination with AUCs of 0.955 (95% CI 0.926-0.983) and 0.905 (95% CI 0.832-0.978) for the training and validation cohorts, respectively. The model achieved a maximum Youden index of 0.7789 with an optimal threshold of 0.3958.
Conclusion: Our multimodal predictive model integrates clinicopathological profiles with imaging biomarkers (ultrasound and magnetic resonance imaging). This model holds promise for preoperative axillary risk stratification in breast cancer patients, thereby identifying candidates suitable for axillary biopsy exemption, while its application serves as a reference for personalized and refined axillary management.
Keywords: Axillary lymph node status; Multimodal model; Noninvasive; Ultrasound-guided biopsy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The studies involving human participants were reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University (XJTU1AF2024LSYY-503). In accordance with national legislation and institutional requirements, written informed consent for participation was not deemed necessary for this study. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
Developing and Evaluating a Nomogram Model Predicting Axillary Lymph Node Metastasis of Triple-Negative Breast Cancer Based on Multimodal Imaging Characteristics.Acad Radiol. 2025 Aug;32(8):4382-4394. doi: 10.1016/j.acra.2025.04.031. Epub 2025 May 15. Acad Radiol. 2025. PMID: 40379590
-
A Validated Ultrasound-Based Scoring System to Stratify Risk of Axillary Metastasis in Breast Cancer: AX-RADS (Axillary Imaging Reporting and Data System).J Surg Oncol. 2025 Jul;132(1):28-34. doi: 10.1002/jso.28159. Epub 2025 May 20. J Surg Oncol. 2025. PMID: 40392181
-
Establishment of an interpretable MRI radiomics-based machine learning model capable of predicting axillary lymph node metastasis in invasive breast cancer.Sci Rep. 2025 Jul 18;15(1):26030. doi: 10.1038/s41598-025-10818-0. Sci Rep. 2025. PMID: 40676103 Free PMC article.
-
Positron emission tomography (PET) and magnetic resonance imaging (MRI) for the assessment of axillary lymph node metastases in early breast cancer: systematic review and economic evaluation.Health Technol Assess. 2011 Jan;15(4):iii-iv, 1-134. doi: 10.3310/hta15040. Health Technol Assess. 2011. PMID: 21276372 Free PMC article.
-
Meta-analysis of ultrasound-guided biopsy of suspicious axillary lymph nodes in the selection of patients with extensive axillary tumour burden in breast cancer.Br J Surg. 2015 Feb;102(3):159-68. doi: 10.1002/bjs.9663. Epub 2014 Oct 29. Br J Surg. 2015. PMID: 25354962
References
-
- Rojas K, Stuckey A. Breast cancer epidemiology and risk factors. Clin Obstet Gynecol. 2016;59(4):651–72. - PubMed
-
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–63. - PubMed
-
- Chida T, Miura Y, Cabral H, Nomoto T, Kataoka K, Nishiyama N. Epirubicin-loaded polymeric micelles effectively treat axillary lymph nodes metastasis of breast cancer through selective accumulation and pH-triggered drug release. J Control Release. 2018;292:130–40. - PubMed
MeSH terms
Grants and funding
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- 82172798/National Natural Science Foundation of China
- No.2024SF-YBXM-223/the Key Research and development Plans in Shaanxi Province of China
- No.2024SF-YBXM-223/the Key Research and development Plans in Shaanxi Province of China
LinkOut - more resources
Full Text Sources
Medical
Research Materials
