

Functional brain activity in persistent postural-perceptual dizziness (PPPD) during galvanic vestibular stimulation reveals sensitization in the multisensory vestibular cortical network
- PMID: 40717118
- PMCID: PMC12301453
- DOI: 10.1038/s41598-025-11529-2
Functional brain activity in persistent postural-perceptual dizziness (PPPD) during galvanic vestibular stimulation reveals sensitization in the multisensory vestibular cortical network
Abstract
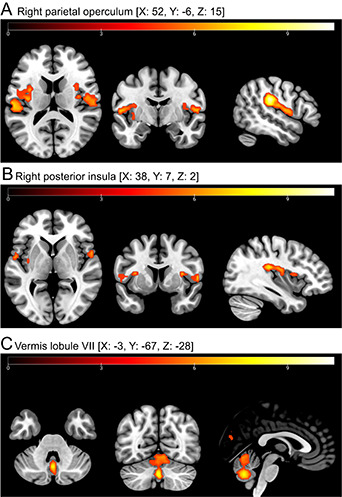
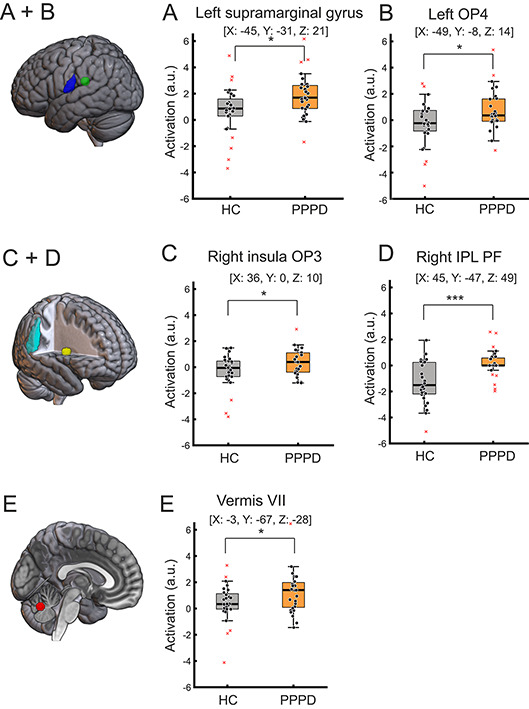
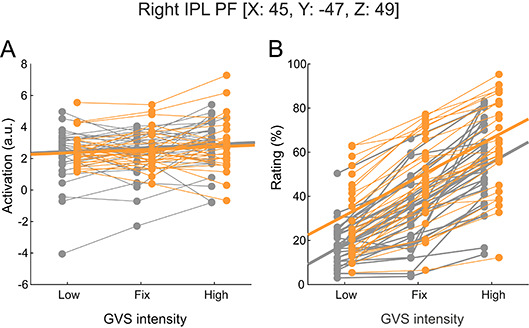
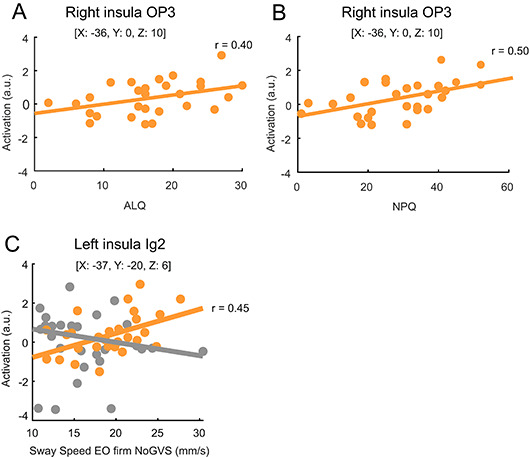
Persistent postural-perceptual dizziness (PPPD) is often preceded by vestibular disorders. We applied galvanic vestibular stimulation (GVS) and related stimulus-evoked activity to individual ratings of perceived motion for each stimulus and to perceived egomotion thresholds by GVS and behavioural parameters outside the scanner: levels of functional disability by standardized questionnaires, visual motion coherence, passive egomotion perception by chair rotation and quantitative postural stability. We hypothesized that the preceding vestibular disorder predisposes to abnormal brain excitability by vestibular stimulation. All participants showed normal vestibular function tests on quantitative testing. GVS with different intensities was applied to 28 patients and 28 age- and gender-matched healthy participants (HC) in the scanner. After each stimulus, participants rated their perceived level of egomotion. GVS perception threshold was significantly lower in PPPD patients. Contrasting stimulus-identical GVS against a sham stimulus, group comparison revealed a stronger activation in the patient's supramarginal gyrus, insular cortex (operculum 3), and vermis. This stronger excitability was not related to the individual threshold of perceived egomotion by GVS. Patients rated GVS-evoked egomotion intensity by identical GVS intensities larger than HC but neural activity did not correlate with individual ratings of perceived egomotion by GVS. As GVS evoked larger egomotion and larger brain activation in patients, the ratio of brain activity to egomotion perception was not different between groups. GVS-evoked insular activity increased with the level of PPPD-related disability and postural imbalance. The larger activation in multisensory cortical vestibular network indicates a sensitization to vestibular stimuli eliciting egomotion perception which increases with levels of PPPD disability. It seems to reflect a sensory-neural amplification rather than an abnormal sensory-perceptual scaling.
Keywords: GVS; PPPD; Persistent postural-perceptual dizziness; Vestibular perception; fMRI.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Visual and vestibular motion perception in persistent postural-perceptual dizziness (PPPD).J Neurol. 2024 Jun;271(6):3227-3238. doi: 10.1007/s00415-024-12255-x. Epub 2024 Mar 5. J Neurol. 2024. PMID: 38441610 Free PMC article.
-
Postural motion perception during vestibular stimulation depends on the motion perception threshold in persistent postural-perceptual dizziness.J Neurol. 2024 Aug;271(8):4909-4924. doi: 10.1007/s00415-024-12415-z. Epub 2024 May 15. J Neurol. 2024. PMID: 38748235 Free PMC article.
-
Postural control during galvanic vestibular stimulation in patients with persistent perceptual-postural dizziness.J Neurol. 2019 May;266(5):1236-1249. doi: 10.1007/s00415-019-09255-7. Epub 2019 Feb 26. J Neurol. 2019. PMID: 30809703
-
Non-pharmacological interventions for persistent postural-perceptual dizziness (PPPD).Cochrane Database Syst Rev. 2023 Mar 13;3(3):CD015333. doi: 10.1002/14651858.CD015333.pub2. Cochrane Database Syst Rev. 2023. PMID: 36912784 Free PMC article.
-
Pharmacological interventions for persistent postural-perceptual dizziness (PPPD).Cochrane Database Syst Rev. 2023 Mar 9;3(3):CD015188. doi: 10.1002/14651858.CD015188.pub2. Cochrane Database Syst Rev. 2023. PMID: 36906836 Free PMC article.
References
-
- Staab, J. P. & Bronstein, A. Behavioural neuro-otology. Oxford Textbook vertigo Imbalance, 333–346 (2013).
-
- Trinidade, A. et al. Predictors of persistent postural-perceptual dizziness (PPPD) and similar forms of chronic Dizziness precipitated by peripheral vestibular disorders: a systematic review. J. Neurol. Neurosurg. Psychiatry94, 904–915 (2023). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
