

Non-Invasive Diagnosis and Monitoring of Diabetic Nephropathy: Assessment of Renal Function and Fibrosis by Diffusion Kurtosis Imaging
- PMID: 40717819
- PMCID: PMC12297023
- DOI: 10.2147/IJGM.S517683
Non-Invasive Diagnosis and Monitoring of Diabetic Nephropathy: Assessment of Renal Function and Fibrosis by Diffusion Kurtosis Imaging
Abstract
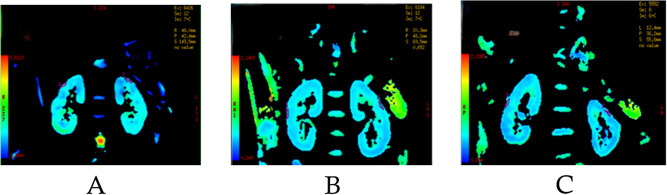
Background: This monocentric, cross-sectional study explored the use of diffusion kurtosis imaging (DKI) as a non-invasive means to diagnose and monitor diabetic nephropathy (DN).
Methods: Patients with diabetes mellitus (DM, n = 11), mild DN (N = 14), and severe DN (n = 29) were recruited. Eight DKI metrics (MK, MD, Da, Dr, Ka, Kr, FA, FAk) were determined from the imaging results, and their correlations with routine laboratory results were analyzed. The receiver operating characteristic (ROC) curves were plotted, and the diagnostic value of the DKI metrics was analyzed. In addition, renal biopsy was carried out for ten DN patients who had appropriate indications. Their interstitial fibrosis and tubular atrophy (IFTA) score and the fibrosis ratio of cortical area (F%) were analyzed in combination with the DKI metrics.
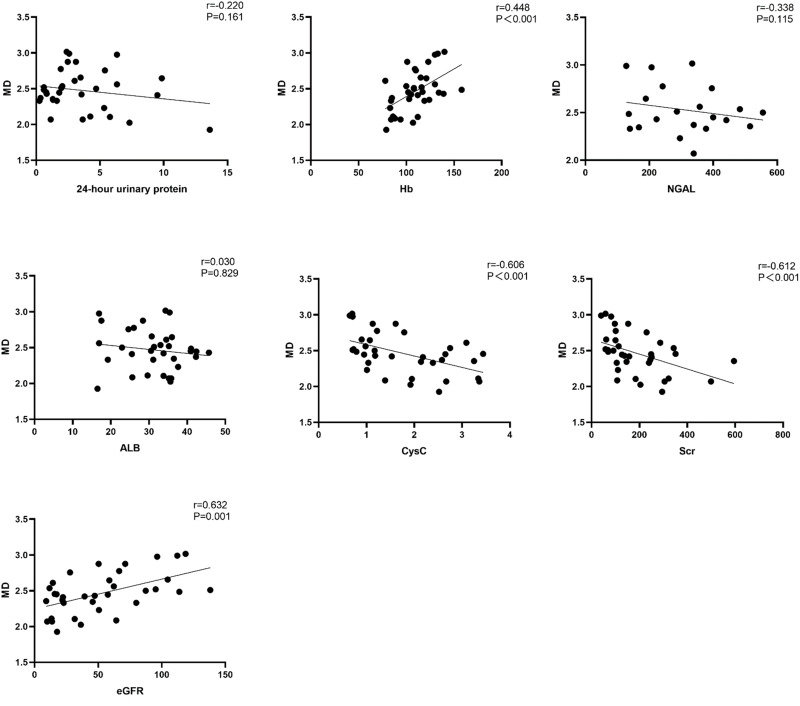
Results: The progression of DN, reflected by the estimated glomerular filtration rate (eGFR), was accompanied by rising mean kurtosis (MK) and axial kurtosis (Ka) along with decreasing mean diffusivity (MD), axial diffusivity (Da), and radial diffusivity (Dr). Whereas MK was correlated negatively with hemoglobin (Hb) and eGFR and positively with neutrophil gelatinase-associated lipocalin (NGAL), cystatin C (CysC), and serum creatinine (Scr), MD, Da, and Dr were positively correlated with Hb and eGFR and negatively correlated with CysC and Scr. For the biopsied patients, MK was positively correlated with IFTA, and fractional anisotropy of kurtosis (FAk) was negatively correlated with F% and IFTA. Among the DKI indicators, MK had the highest AUC (0.922, 95% CI: 0.843-1.000).
Conclusion: The noninvasive monitoring of DN was feasible with DKI, and MK could indicate the renal function and fibrosis of DN patients. Changes in MK may also serve as a biomarker to assess treatment response (eg, microstructural improvement) after therapeutic interventions (eg, drug therapy for diabetic nephropathy, anti-fibrotic therapy).
Keywords: diabetes mellitus; diabetic nephropathy; diffusion kurtosis imaging; magnetic resonance imaging; mean kurtosis.
Plain language summary
Diabetic nephropathy (DN) is a serious kidney complication of diabetes and the leading cause of end-stage renal disease. While imaging tools like ultrasound, CT, and standard MRI are widely used to evaluate kidney structure and blood flow, they play a limited role in diagnosing or monitoring DN. There is a growing need for non-invasive methods that can detect early changes and track disease progression more precisely. Diffusional Kurtosis Imaging (DKI) is an advanced MRI technique that captures the complexity of water movement in tissues, offering insights into kidney microstructure. The present study analyzed, in DN patients, eight DKI metrics—mean kurtosis and diffusivity (MK and MD), axial and radial diffusivity and kurtosis (Da, Dr, Ka, Kr,), fractional anisotropy (FA), and fractional anisotropy in kurtosis (FAk)—and compared them to standard lab markers and biopsy results. Among all DKI measures, MK showed the strongest correlation with kidney function and fibrosis. Specifically, higher MK values were associated with worse kidney function (lower hemoglobin and eGFR, higher creatinine, NGAL, and cystatin C) and more severe tissue damage (higher fibrosis scores on biopsy). MK also achieved the highest diagnostic accuracy (AUC = 0.922) in distinguishing disease severity. These findings suggest that DKI, and MK in particular, can serve as a powerful, non-invasive biomarker for assessing kidney damage and fibrosis in DN patients. MK may also help track treatment response, offering a way to monitor improvements in kidney microstructure following therapies.
© 2025 Yuan et al.
Conflict of interest statement
The authors declare no conflicts of interest in this work.
Figures






Similar articles
-
Non-invasive assessment of early stage diabetic nephropathy by DTI and BOLD MRI.Br J Radiol. 2020 Jan;93(1105):20190562. doi: 10.1259/bjr.20190562. Epub 2019 Oct 25. Br J Radiol. 2020. PMID: 31603347 Free PMC article.
-
Prospective evaluation of arterial spin labeling and diffusion tensor imaging-magnetic resonance imaging for the non-invasive assessment of renal allograft dysfunction.Quant Imaging Med Surg. 2025 Aug 1;15(8):6882-6896. doi: 10.21037/qims-2025-604. Epub 2025 Jul 29. Quant Imaging Med Surg. 2025. PMID: 40785929 Free PMC article.
-
Translating state-of-the-art spinal cord MRI techniques to clinical use: A systematic review of clinical studies utilizing DTI, MT, MWF, MRS, and fMRI.Neuroimage Clin. 2015 Dec 4;10:192-238. doi: 10.1016/j.nicl.2015.11.019. eCollection 2016. Neuroimage Clin. 2015. PMID: 26862478 Free PMC article.
-
Non-invasive MRI-based assessment of reactive stromal grade in prostate cancer using diffusion kurtosis imaging and stretched-exponential model.BMC Med Imaging. 2025 Aug 19;25(1):339. doi: 10.1186/s12880-025-01881-0. BMC Med Imaging. 2025. PMID: 40830853 Free PMC article.
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
