

Real-Time Postural Feedback to Optimize Ergonomics and Musculoskeletal Health in Ophthalmology Residents: A Canadian Pilot Quality Improvement Study
- PMID: 40717881
- PMCID: PMC12292650
- DOI: 10.7759/cureus.88736
Real-Time Postural Feedback to Optimize Ergonomics and Musculoskeletal Health in Ophthalmology Residents: A Canadian Pilot Quality Improvement Study
Abstract
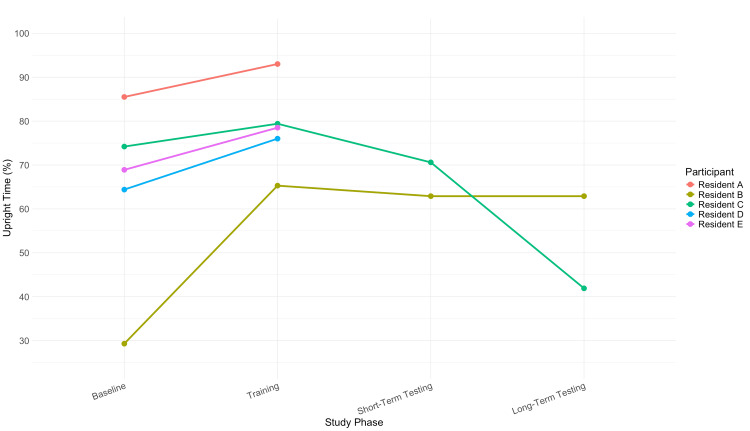
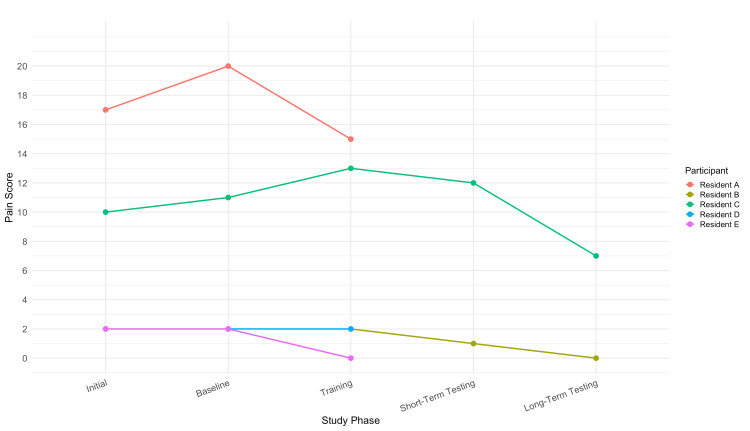
Background Musculoskeletal (MSK) pain is a common occupational concern in ophthalmology, often associated with the sustained and ergonomically demanding positions required during clinical and surgical activities. Tasks such as slit-lamp examinations, indirect ophthalmoscopy, and microscope-assisted procedures may contribute to postural strain. Despite this, ergonomics remains an underemphasized component of resident education, even though physical strain during training can influence long-term clinical performance and physician well-being. This pilot study investigates whether the UPRIGHT GO 2, a wearable posture trainer, can improve posture and reduce MSK pain in ophthalmology residents. Methodology This prospective, interventional, proof-of-concept case series recruited five postgraduate year (PGY) 2 to 5 ophthalmology residents at McMaster University. Each participant wore the UPRIGHT GO 2 device over the following four distinct two-week phases: baseline, training, short-term testing, and long-term testing. During the baseline phase, the vibration mode was turned off to establish baseline posture data. In the training phase, the vibration mode was activated with a 30-second delay to provide real-time posture feedback. The short-term testing phase was conducted with the vibration turned off to assess short-term retention effects. The long-term testing phase, also with vibration off, was performed six weeks after short-term testing to evaluate long-term effects. All participants attended a brief standardized educational session before device use, which reviewed ergonomic principles relevant to ophthalmology, including optimal posture during slit-lamp examinations, indirect ophthalmoscopy, and microscope-guided procedures. The primary outcome was the percent time spent in an upright posture. The secondary outcome was MSK pain, assessed using a modified Nordic musculoskeletal and numerical pain rating scale. Results All participants (N = 5, 100%) completed the baseline and training phases, with two residents (n = 2, 40%) completing the full study through long-term testing. The mean proportion of time spent in an upright posture increased from 68.9% at baseline to 78.5% during the training phase, coinciding with the activation of vibration-based feedback. This improvement declined to 66.8% during short-term testing and further to 52.4% at long-term follow-up (n = 2, 40%), suggesting a potential attenuation of effect in the absence of continued reinforcement. MSK pain scores followed a similar pattern: mean scores increased slightly from 6.6 to 7.4 post-baseline, then declined post-training (6.4), post-short-term testing (6.5), and reached their lowest average at long-term follow-up (3.5, n = 2, 40%). All participants demonstrated either stable or improved pain scores, with two residents exhibiting concordant improvements in both posture and pain. These findings suggest that wearable feedback devices may enhance ergonomics and mitigate MSK symptoms among ophthalmology residents when incorporated into clinical training environments. Conclusions The UPRIGHT GO 2, combined with an educational intervention, may provide short-term ergonomic benefit for posture and MSK pain in ophthalmology residents. However, long-term posture retention varied. Limitations include the small sample size and device data fidelity. Larger studies are needed to validate these findings and guide ergonomic strategies in medical training.
Keywords: clinical ergonomics; medical trainee wellness; musculoskeletal pain; ophthalmology residents; physician well-being; postural biofeedback; posture monitoring; quality improvement; resident education; wearable posture device.
Copyright © 2025, Bolis et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Hamilton Integrated Research Ethics Board issued approval 16005. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Workplace interventions for reducing sitting at work.Cochrane Database Syst Rev. 2018 Jun 20;6(6):CD010912. doi: 10.1002/14651858.CD010912.pub4. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2018 Dec 17;12:CD010912. doi: 10.1002/14651858.CD010912.pub5. PMID: 29926475 Free PMC article. Updated.
-
Use of endoanal ultrasound for reducing the risk of complications related to anal sphincter injury after vaginal birth.Cochrane Database Syst Rev. 2015 Oct 29;2015(10):CD010826. doi: 10.1002/14651858.CD010826.pub2. Cochrane Database Syst Rev. 2015. PMID: 26513224 Free PMC article.
References
-
- Symptoms of musculoskeletal disorders in ophthalmologists. Dhimitri KC, McGwin G Jr, McNeal SF, et al. Am J Ophthalmol. 2005;139:179–181. - PubMed
-
- Survey of occupational musculoskeletal pain and injury in Canadian ophthalmology. Diaconita V, Uhlman K, Mao A, Mather R. Can J Ophthalmol. 2019;54:314–322. - PubMed
LinkOut - more resources
Full Text Sources