

Comparison of Long-Term Outcomes Between Repeated Hepatic Resection and Radiofrequency Ablation in Patients with Small Recurrent Hepatocellular Carcinoma After Initial Curative Resection: A Propensity Score Matched Study
- PMID: 40718075
- PMCID: PMC12296703
- DOI: 10.2147/JHC.S496470
Comparison of Long-Term Outcomes Between Repeated Hepatic Resection and Radiofrequency Ablation in Patients with Small Recurrent Hepatocellular Carcinoma After Initial Curative Resection: A Propensity Score Matched Study
Abstract
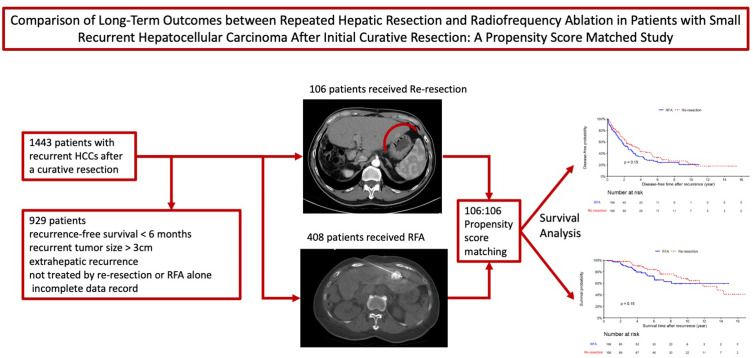
Background: Repeat hepatic resection (re-resection) and radiofrequency ablation (RFA) are both standard treatments for small recurrent hepatocellular carcinoma (HCC) after curative resection. This study compares long-term outcomes of these treatments.
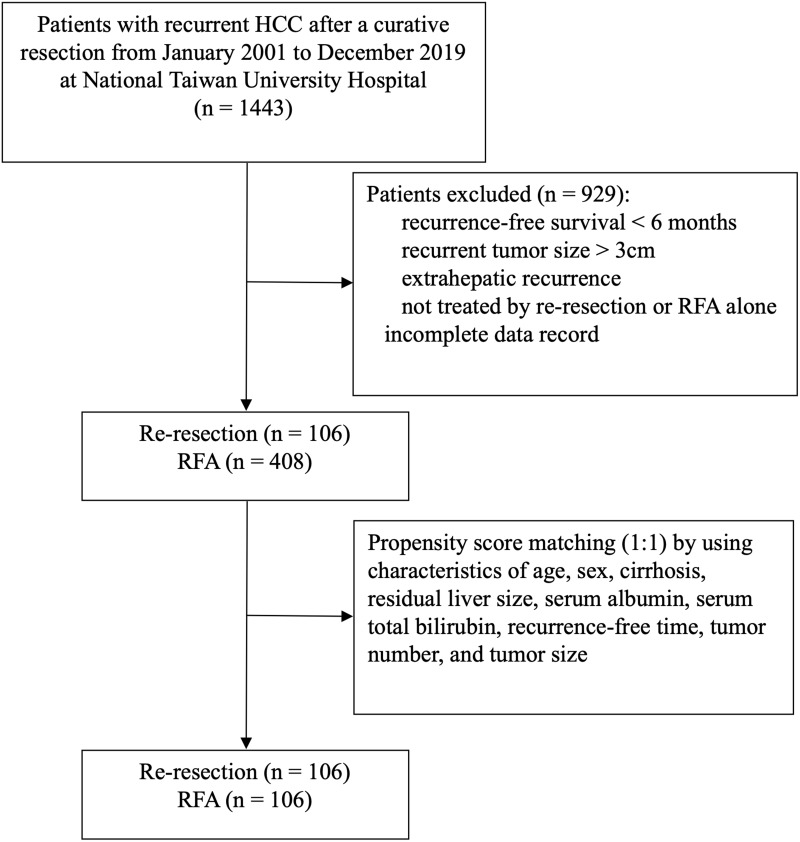
Methods: This retrospective study included patients with recurrent HCC smaller than 3 cm treated with re-resection or RFA from 2001 to 2019 in a tertiary center. Propensity score matching (PSM) minimized baseline differences. Primary outcomes were overall survival (OS) and disease-free survival (DFS). Subgroup analyses explored outcomes based on recurrence interval, hepatitis infection status, and RFA guidance method (ultrasound [US] versus computed tomography [CT]). Multivariate Cox regression identified predictors of survival and secondary recurrence.
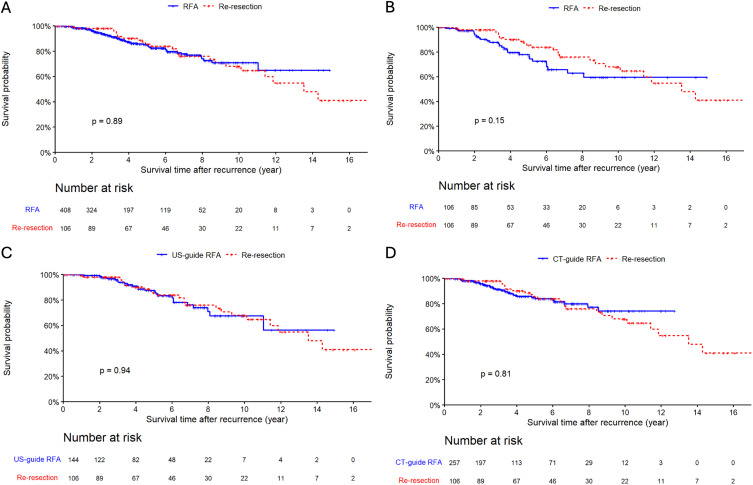
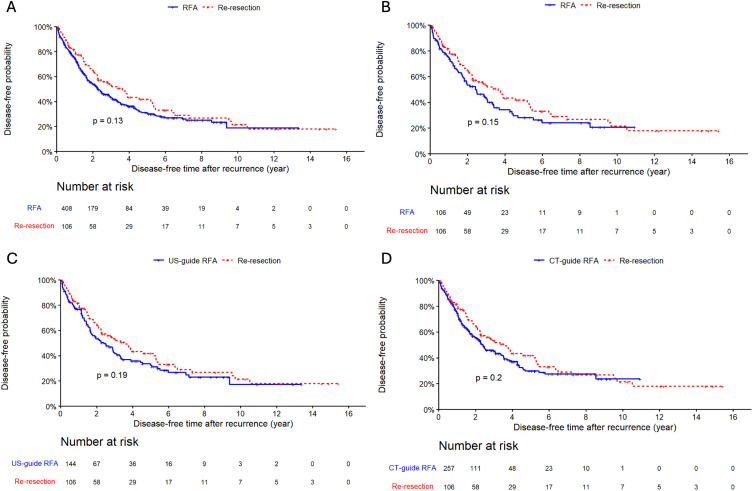
Results: After PSM, 106 patients in the re-resection group and 106 in the RFA group were compared. OS rates at 3, 5, and 8 years for re-resection were 97.9%, 85.4%, and 75.8%, compared to 87.8%, 77.9%, and 62.8% for RFA (p = 0.15). DFS rates were 53.3%, 41.8%, and 26.7% for re-resection versus 43.9%, 28.1%, and 24.0% for RFA (p = 0.15). Subgroup analysis indicated re-resection was superior in early recurrence (<24 months) and HBV-related HCC. US-guided and CT-guided RFA showed no significant differences in OS or DFS. HCV infection and multiple tumors were independent predictors of secondary recurrence.
Conclusion: Repeat hepatic resection and RFA offer comparable survival for small recurrent HCC. Re-resection is preferred for early recurrence and HBV-related HCC. US- and CT-guided RFA are equally effective alternatives.
Keywords: hepatocellular carcinoma; outcome; radiofrequency ablation; recurrence; repeat resection.
© 2025 Hsiao et al.
Conflict of interest statement
All author declared no conflict of interest.
Figures
Similar articles
-
Comparison of Computed Tomography and Ultrasound-Guided Radiofrequency Ablation for Recurrent Subdiaphragmatic Hepatocellular Carcinoma After Resection.J Hepatocell Carcinoma. 2025 Jun 27;12:1231-1240. doi: 10.2147/JHC.S524399. eCollection 2025. J Hepatocell Carcinoma. 2025. PMID: 40599642 Free PMC article.
-
Long-Term Outcome of Repeat Resection versus Radiofrequency Ablation for Intrahepatic Recurrence after Curative Resection of Hepatocellular Carcinoma Initially within Barcelona Clinic Liver Cancer Staging System 0-A Stages: A Multicenter Study.Dig Dis. 2025 Jun 24:1-14. doi: 10.1159/000546743. Online ahead of print. Dig Dis. 2025. PMID: 40555206
-
Competing risk analysis of surgical resection vs. radiofrequency ablation in early-stage small hepatocellular carcinoma: a SEER-based study.Transl Cancer Res. 2025 Jun 30;14(6):3565-3576. doi: 10.21037/tcr-2024-2550. Epub 2025 Jun 27. Transl Cancer Res. 2025. PMID: 40687222 Free PMC article.
-
Radiofrequency (thermal) ablation versus no intervention or other interventions for hepatocellular carcinoma.Cochrane Database Syst Rev. 2013 Dec 19;2013(12):CD003046. doi: 10.1002/14651858.CD003046.pub3. Cochrane Database Syst Rev. 2013. PMID: 24357457 Free PMC article.
-
Ablative and non-surgical therapies for early and very early hepatocellular carcinoma: a systematic review and network meta-analysis.Health Technol Assess. 2023 Dec;27(29):1-172. doi: 10.3310/GK5221. Health Technol Assess. 2023. PMID: 38149643 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
