

Apical Hypertrophic Cardiomyopathy With Endomyocardial Calcification: A Multimodality Imaging-Based Case Report
- PMID: 40718246
- PMCID: PMC12296395
- DOI: 10.7759/cureus.86822
Apical Hypertrophic Cardiomyopathy With Endomyocardial Calcification: A Multimodality Imaging-Based Case Report
Abstract
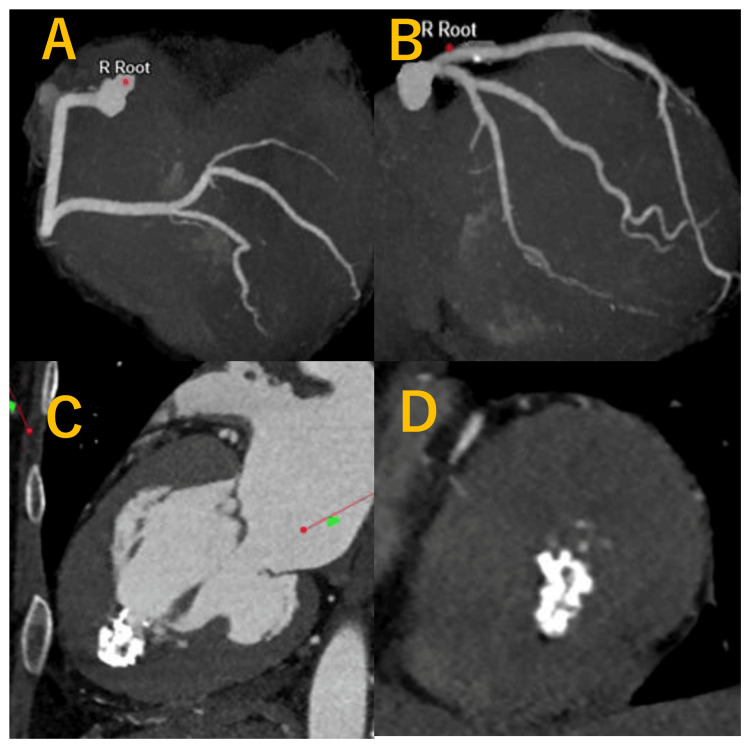
Apical hypertrophic cardiomyopathy (ApHCM) with endomyocardial calcification has been reported in only a small number of cases, making its imaging features less well established. We describe a 53-year-old woman with no significant medical history who was referred for further evaluation following abnormal electrocardiographic findings identified during a routine medical check-up. Multimodality imaging, including transthoracic echocardiography, coronary computed tomography angiography, and cardiac magnetic resonance imaging (CMR), demonstrated apical myocardial hypertrophy and endomyocardial calcification, establishing the diagnosis of ApHCM with calcific involvement. The pathophysiological mechanism underlying myocardial calcification in ApHCM remains poorly defined. In this case, adenosine stress perfusion CMR and myocardial strain analysis were performed for further characterization. These investigations revealed a circumferential stress-induced perfusion defect predominantly involving the apical myocardium, along with markedly reduced apical global circumferential strain (GCS), suggesting a potential association with chronic subendocardial ischemia; however, this remains a hypothesis based on a single case and requires further validation. The use of adenosine stress perfusion CMR in this case was intended to evaluate for coexisting ischemia, given the presence of calcification and impaired apical strain. Clinically, identifying calcification rather than thrombus is critical, as it may prevent unnecessary anticoagulation and guide appropriate follow-up strategies. This case underscores the importance of a multimodality imaging approach in assessing both structural and functional alterations in atypical phenotypes of hypertrophic cardiomyopathy.
Keywords: apical hcm; cardiovascular magnetic resonance imaging (cmr); endomyocardial calcification; myocardial perfusion reserve; myocardial strain.
Copyright © 2025, Tanabe et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures






Similar articles
-
Apical Hypertrophic Cardiomyopathy: A Clinical & Multimodality Imaging Assessment.Echocardiography. 2025 Jul;42(7):e70235. doi: 10.1111/echo.70235. Echocardiography. 2025. PMID: 40679124 Review.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Systematic review and modelling of the cost-effectiveness of cardiac magnetic resonance imaging compared with current existing testing pathways in ischaemic cardiomyopathy.Health Technol Assess. 2014 Sep;18(59):1-120. doi: 10.3310/hta18590. Health Technol Assess. 2014. PMID: 25265259 Free PMC article.
-
Clinical Characteristics and Cardiac Magnetic Resonance Findings in Patients With Hypertrophic Cardiomyopathy in Brunei Darussalam.Cureus. 2025 Jun 18;17(6):e86303. doi: 10.7759/cureus.86303. eCollection 2025 Jun. Cureus. 2025. PMID: 40688918 Free PMC article.
-
What is the value of routinely testing full blood count, electrolytes and urea, and pulmonary function tests before elective surgery in patients with no apparent clinical indication and in subgroups of patients with common comorbidities: a systematic review of the clinical and cost-effective literature.Health Technol Assess. 2012 Dec;16(50):i-xvi, 1-159. doi: 10.3310/hta16500. Health Technol Assess. 2012. PMID: 23302507 Free PMC article.
References
-
- Comparison of prevalence of apical hypertrophic cardiomyopathy in Japan and the United States. Kitaoka H, Doi Y, Casey SA, Hitomi N, Furuno T, Maron BJ. Am J Cardiol. 2003;92:1183–1186. - PubMed
-
- Call a spade a spade: missed diagnosis of apical hypertrophic cardiomyopathy. Leaphart D, Waring A, Suranyi P, Fernandes V. Am J Med Sci. 2019;358:299–303. - PubMed
-
- Hypertrophic cardiomyopathy with left ventricular apical aneurysm: implications for risk stratification and management. Rowin EJ, Maron BJ, Haas TS, Garberich RF, Wang W, Link MS, Maron MS. J Am Coll Cardiol. 2017;69:761–773. - PubMed
-
- Intramyocardial calcification in a patient with apical hypertrophic cardiomyopathy. Kaimoto S, Kawasaki T, Yamano M, Miki S, Kamitani T, Sugihara H. Intern Med. 2012;51:1523–1526. - PubMed
Publication types
LinkOut - more resources
Full Text Sources