

Primary Pericardial Synovial Sarcoma: A Case Series and Review of Literature
- PMID: 40718269
- PMCID: PMC12293661
- DOI: 10.7759/cureus.86731
Primary Pericardial Synovial Sarcoma: A Case Series and Review of Literature
Abstract
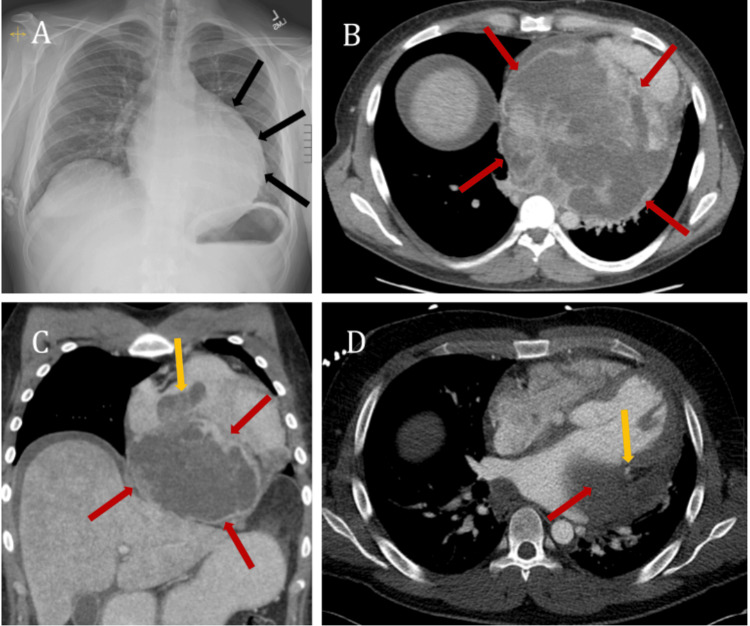
Primary pericardial synovial sarcoma (PPSS) is a rare and aggressive cancer that arises from pluripotent mesenchymal cells of the pericardium. The pathognomonic genetic hallmark is the chromosomal translocation t(X;18)(p11;q11), resulting in the SS18-SSX fusion oncogene, which, down the line, disrupts transcription regulation and chromatin remodeling, ultimately leading to carcinogenesis. In our article, we describe two cases of PPSS in previously healthy young men, managed with multidisciplinary teams, along with a review of the literature of cases reported to date. Both of our patients are young adults, with very different presentations in terms of symptoms, one presenting with shortness of breath (SOB) and the second with chest pain. Both patients had imaging studies that reported a pericardial mass. Ultimately, a diagnostic evaluation was done, with fluorescence in situ hybridization (FISH) confirming primary pericardial synovial sarcoma. Unfortunately, both patients passed away within a week of diagnosis. A comprehensive search of public databases, including PubMed and Google Scholar, was conducted up to 2025. The search criteria included synovial pericardial sarcoma, sarcoma of the heart, cardiac sarcoma, and primary pericardial synovial sarcoma. The search yielded over 100 results, of which 46 articles focused specifically on primary pericardial synovial sarcoma. This article summarizes all reported PPSS cases to date, including patient age, race, gender, symptoms, cytological analysis, and histological subtypes.
Keywords: cardiac tumors; pericardial sarcoma; primary pericardial sarcoma; spindle cell sarcoma; thoracic oncology.
Copyright © 2025, Kaur et al.
Conflict of interest statement
Human subjects: All authors have confirmed that this study did not involve human participants or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures






Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
SS18-SSX and SSX c-terminus antibodies for identification of specific fusion oncoprotein in mesenchymal neoplasms.Pathology. 2025 Aug;57(5):579-584. doi: 10.1016/j.pathol.2024.11.013. Epub 2025 Feb 12. Pathology. 2025. PMID: 40128131
-
Orbital Synovial Sarcoma: Novel Case Report and Review of the Literature.Ophthalmic Plast Reconstr Surg. 2025 Aug 20. doi: 10.1097/IOP.0000000000003038. Online ahead of print. Ophthalmic Plast Reconstr Surg. 2025. PMID: 40833150
-
Can a Liquid Biopsy Detect Circulating Tumor DNA With Low-passage Whole-genome Sequencing in Patients With a Sarcoma? A Pilot Evaluation.Clin Orthop Relat Res. 2025 Jan 1;483(1):39-48. doi: 10.1097/CORR.0000000000003161. Epub 2024 Jun 21. Clin Orthop Relat Res. 2025. PMID: 38905450
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article.
References
-
- Co-existence of SYT-SSX1 and SYT-SSX2 fusions in synovial sarcomas. Yang K, Lui WO, Xie Y, et al. Oncogene. 2002;21:4181–4190. - PubMed
-
- Tumors of the heart and pericardium. McAllister HA Jr, Hall RJ, Cooley DA. Curr Probl Cardiol. 1999;24:59–116. - PubMed
-
- Synovial sarcomas usually metastasize after >5 years: a multicenter retrospective analysis with minimum follow-up of 10 years for survivors. Krieg AH, Hefti F, Speth BM, et al. Ann Oncol. 2011;22:458–467. - PubMed
-
- Primary pericardial tumors. Restrepo CS, Vargas D, Ocazionez D, Martínez-Jiménez S, Betancourt Cuellar SL, Gutierrez FR. Radiographics. 2013;33:1613–1630. - PubMed
Publication types
LinkOut - more resources
Full Text Sources