

A Case in Which the Endoscopic Denker's Approach Was Useful in the Diagnosis of IgG4-Related Ophthalmic Disease
- PMID: 40718310
- PMCID: PMC12296910
- DOI: 10.7759/cureus.86809
A Case in Which the Endoscopic Denker's Approach Was Useful in the Diagnosis of IgG4-Related Ophthalmic Disease
Abstract
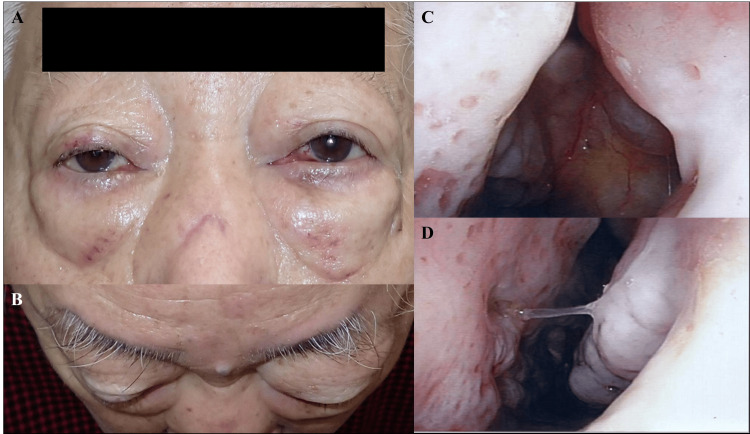
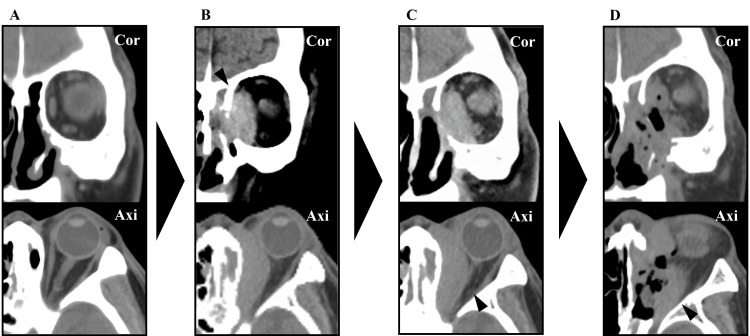
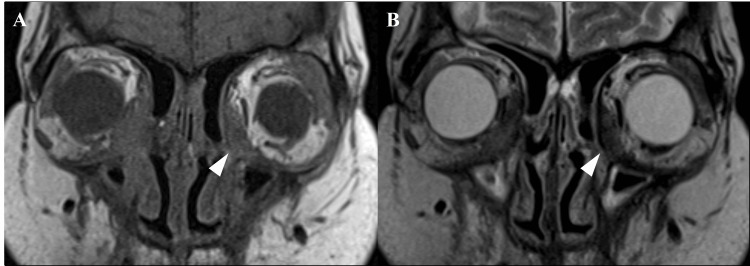
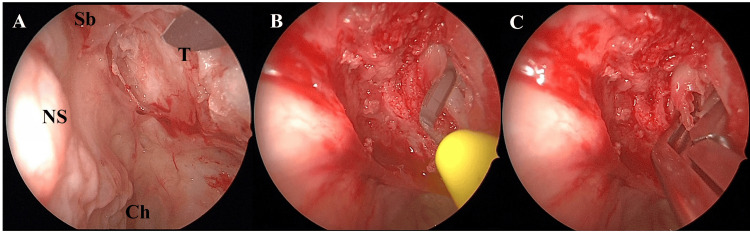
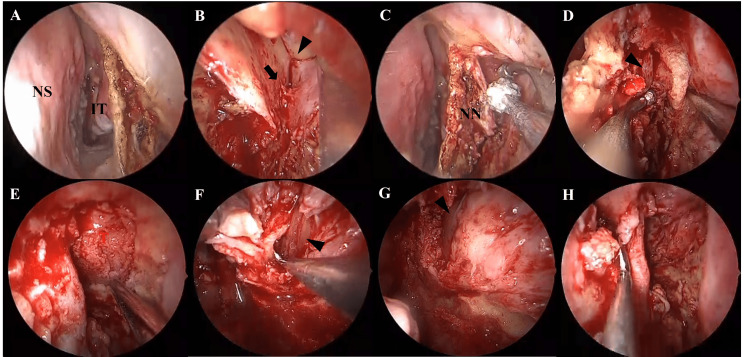
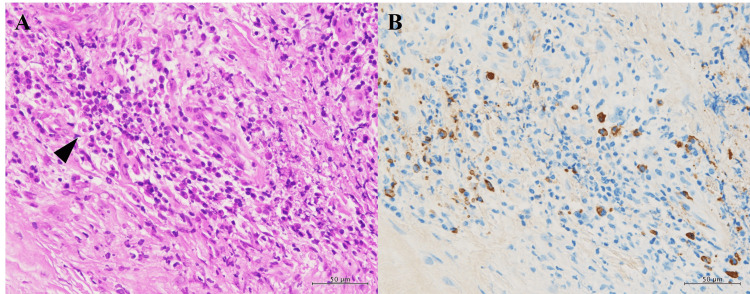
IgG4-related disease (IgG4-RD) is a chronic inflammatory condition characterized by elevated serum IgG4 levels, infiltration of IgG4-positive plasma cells, and fibrosis in various organs. We report the case of a 76-year-old man who presented with left-sided proptosis. Computed tomography revealed a mass lesion in the left orbit. An initial biopsy via a transnasal approach under local anesthesia was inconclusive. Although endoscopic sinus surgery was performed under general anesthesia, a definitive diagnosis could not be obtained. The lesion continued to enlarge, and subsequent ophthalmologic examinations revealed progressive optic nerve compression. Therefore, tumor resection was performed again under general anesthesia using the endoscopic Denker's approach. The tumor was successfully resected without complications. Histopathological findings led to a diagnosis of probable IgG4-related ophthalmic disease (IgG4-ROD). Following surgery, the residual lesion enlarged again; however, a three-day course of steroid pulse therapy resulted in reduction of the lesion and improvement of optic nerve compression. The patient has remained relapse-free. While 81% of IgG4-ROD cases involve the lacrimal gland, other orbital structures such as the pterygopalatine fossa, trigeminal nerve branches, extraocular muscles, orbital fat, eyelids, and nasolacrimal duct can also be affected. In cases without lacrimal gland involvement, the optimal approach for obtaining diagnostic biopsy specimens should be considered individually. Although there is no consensus on the required volume of tissue for diagnosis, we believe that aggressive resection of the central lesion is necessary for accurate diagnosis. The endoscopic Denker's approach facilitates wide exposure and resection of far lateral maxillary sinus lesions, enabling both decompression and definitive diagnosis, which can lead to appropriate subsequent treatment.
Keywords: endoscopic sinus surgery; optic nerve compression; orbital tumor; probable; steroids.
Copyright © 2025, Yamaguchi et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Surgical orbital decompression for thyroid eye disease.Cochrane Database Syst Rev. 2011 Dec 7;(12):CD007630. doi: 10.1002/14651858.CD007630.pub2. Cochrane Database Syst Rev. 2011. PMID: 22161415
-
IgG4-related disease presenting as central skull base osteomyelitis with deep neck abscesses: A case report.Medicine (Baltimore). 2025 Jul 18;104(29):e43351. doi: 10.1097/MD.0000000000043351. Medicine (Baltimore). 2025. PMID: 40696699 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Probing for congenital nasolacrimal duct obstruction.Cochrane Database Syst Rev. 2017 Jul 12;7(7):CD011109. doi: 10.1002/14651858.CD011109.pub2. Cochrane Database Syst Rev. 2017. PMID: 28700811 Free PMC article.
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.
References
-
- New insights into chronic rhinosinusitis associated with IgG4-related disease. Takano K, Kamekura R, Okuni T, Yamamoto K. Auris Nasus Larynx. 2024;51:356–360. - PubMed
-
- IgG4-related respiratory disease. Matsui S. Mod Rheumatol. 2019;29:251–256. - PubMed
-
- Location and frequency of lesions in patients with IgG4-related ophthalmic diseases. Sogabe Y, Ohshima K, Azumi A, et al. Graefes Arch Clin Exp Ophthalmol. 2014;252:531–538. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous