

Unreactive EEG Background Is Associated With Unfavorable Outcome in Patients With Disorders of Consciousness of Various Etiologies: An Adult Cohort Study
- PMID: 40718992
- PMCID: PMC12301862
- DOI: 10.1111/ene.70312
Unreactive EEG Background Is Associated With Unfavorable Outcome in Patients With Disorders of Consciousness of Various Etiologies: An Adult Cohort Study
Abstract
Objective: Prognostication of neurological outcome in critically ill patients presents significant challenges. While EEG reactivity may be associated with outcome in hypoxic-ischemic brain injury (HIBI), it has received scarce attention in other etiological conditions. Our objective was to investigate the association of EEG reactivity to clinical outcome in patients with disorders of consciousness of various etiologies.
Method: This is an ancillary study of the randomized CERTA trial (NCT03129438), which included adults with disorders of consciousness randomized to continuous EEG for 30-48 h or two routine EEGs (20-30 min). We explored the association between EEG characteristics and neurological outcome at 6 months, a modified Rankin Scale (mRS) 3-6 being considered unfavorable.
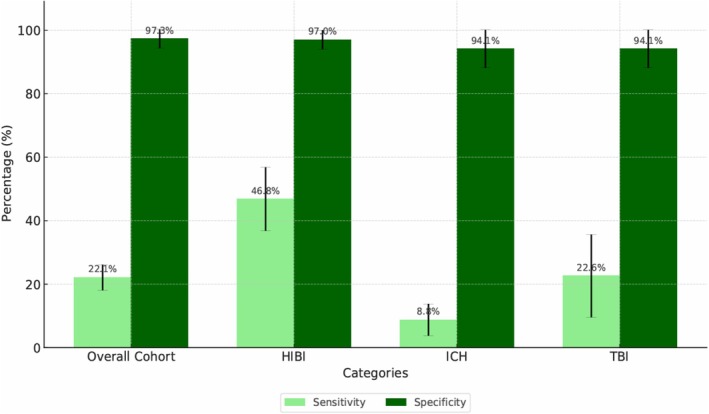
Results: A total of 364 patients were included. Among them, 112 patients had HIBI, 85 intracranial hemorrhage (ICH), 28 ischemic stroke, 48 traumatic brain injury (TBI), 23 toxic-metabolic encephalopathy, 7 encephalitis, and 114 had unknown or other etiologies. In the overall cohort, abnormal background continuity (OR 2.33, 95% CI [1.15-4.76], p = 0.019), ictal-interictal continuum features (OR 2.78, 95% CI [1.16-6.67], p = 0.021) and unreactive background (OR 10.9, 95% CI [1.97-58.82], p = 0.006) were independently associated with unfavorable outcome. In the overall cohort, unreactive EEG had specificity of 97.3% (95% CI [94.3-100]) and sensitivity of 22.1% (95% CI [17-27.2]) for unfavorable outcome. In HIBI, specificity was 97% (95% CI [91.1-100]) and sensitivity 46.8% (95% CI [35.8-57.8]); in ICH, specificity was 94.1% (95% CI [83-100]) and sensitivity 8.8% (95% CI [2.05-15.55]); in TBI, specificity was 94.1% (95% CI [83-100]) and sensitivity 22.6% (95% CI [7.8-37.3]).
Conclusion: In this etiologically mixed cohort of critically ill adults, unreactive EEG predicted unfavorable outcome at 6 months with high specificity. EEG reactivity may reduce prognostic uncertainty not only for patients with HIBI, but also for other types of acute brain injury, such as TBI and ICH.
Keywords: EEG reactivity; cardiac arrest; intracranial hemorrhage; neuroprognostication; traumatic brain injury.
© 2025 The Author(s). European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Sex as a prognostic factor for mortality in adults with acute symptomatic pulmonary embolism.Cochrane Database Syst Rev. 2025 Mar 20;3(3):CD013835. doi: 10.1002/14651858.CD013835.pub2. Cochrane Database Syst Rev. 2025. PMID: 40110896
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
