

Relative change rate of liver stiffness measurements predicts the risk of liver decompensation in compensated advanced chronic liver disease
- PMID: 40719905
- PMCID: PMC12304040
- DOI: 10.1007/s10238-025-01813-w
Relative change rate of liver stiffness measurements predicts the risk of liver decompensation in compensated advanced chronic liver disease
Abstract
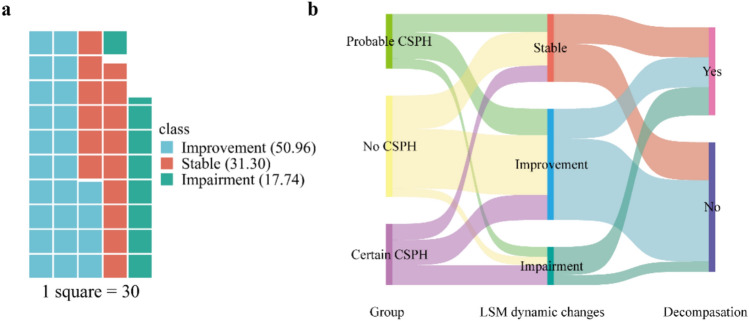
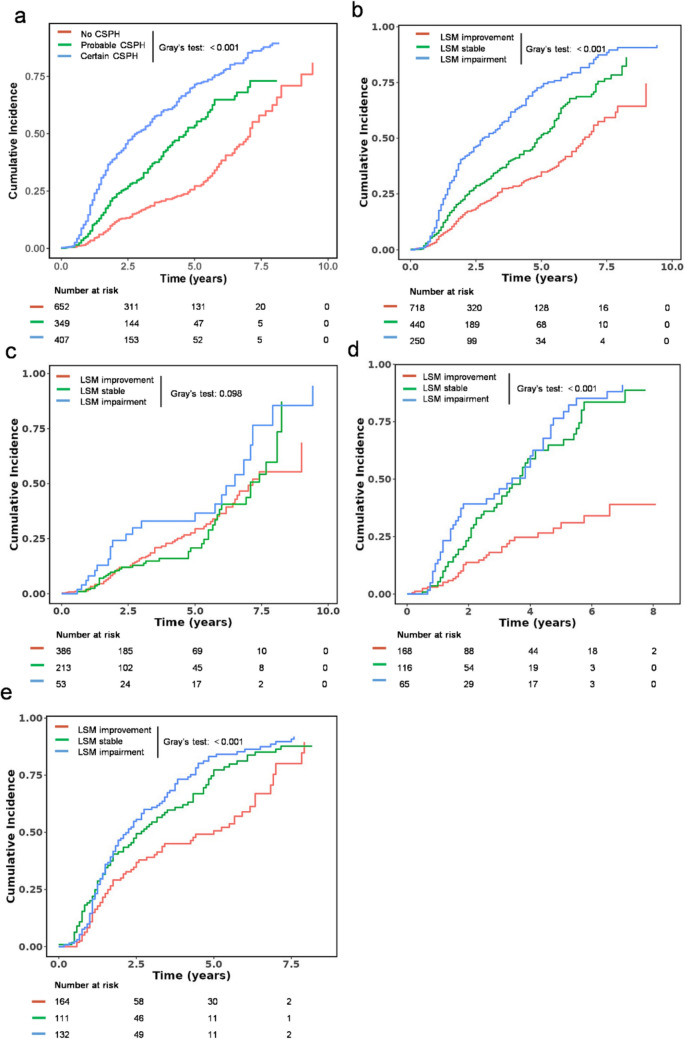
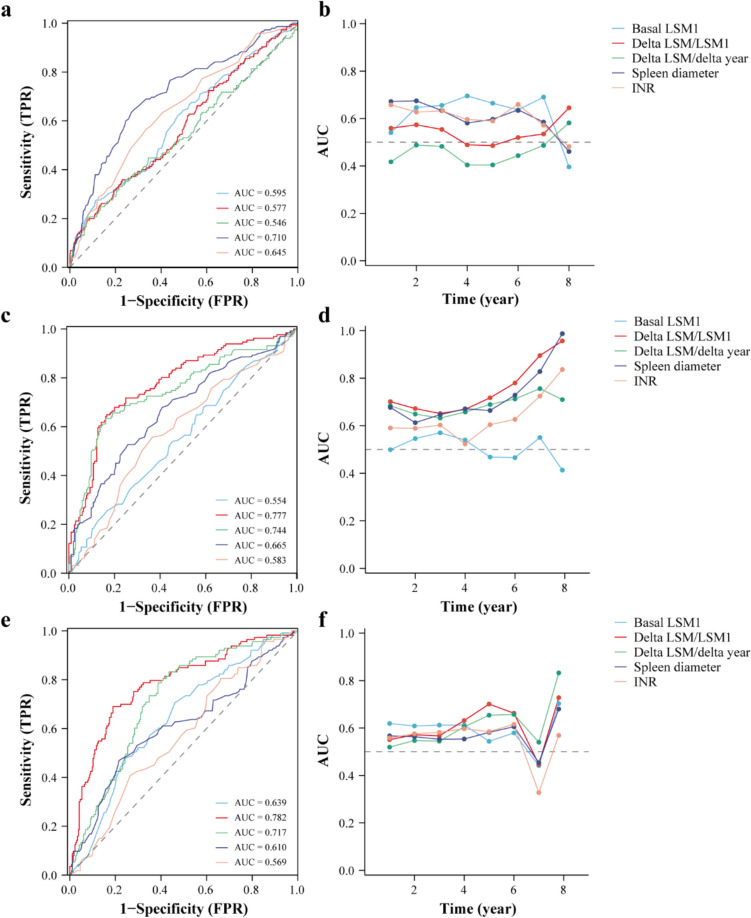
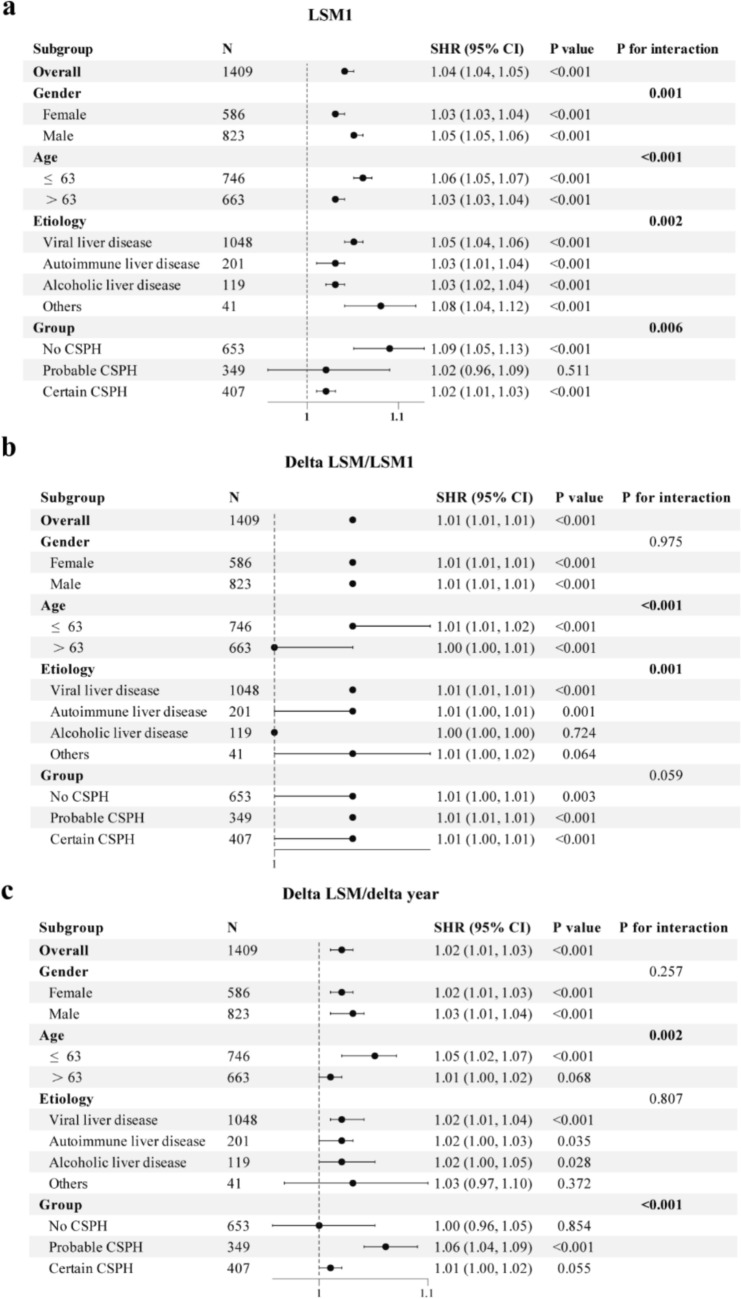
Patients with compensated advanced chronic liver disease (cACLD) have a significant risk of decompensation. Therefore, this study aimed to evaluate the predictive value of dynamic liver stiffness measurements (LSM) for decompensation risk, and their performance across different clinically significant portal hypertension (CSPH) risk stratification. This retrospective cohort study included 1409 patients with cACLD. Patients were divided into no CSPH, probable CSPH, and certain CSPH groups. Competing risk regression analysis was used to identify the independent predictors. The receiver operating characteristic curve and time-dependent area under the curve were used to evaluate the predictive performance. During follow-up, liver decompensation incidence increased with CSPH severity (22.2% with no CSPH, 37.5% with probable CSPH, and 64.9% with certain CSPH, p < 0.001). Multivariate regression analysis identified age, basal LSM1, delta LSM/LSM1, delta LSM/delta year, spleen diameter, and international normalized ratio as independent risk factors for liver decompensation. In the no CSPH group, spleen diameter showed the best predictive ability (AUC = 0.710). For probable and certain CSPH groups, delta LSM/LSM1 showed superior predictive performance (AUC: 0.777 and 0.782, respectively). The predictive power of basal LSM1 was relatively limited across all groups (AUC: 0.554-0.639). Subgroup analysis revealed interactions between age, sex, different etiologies, and CSPH subgroups. The relative change rate of LSM outperformed basal LSM1 and annual change rate in predicting liver decompensation risk, particularly in patients with existing portal hypertension. Dynamic assessments and differentiated prediction strategies are essential for optimal patient managements.
Keywords: Clinically significant portal hypertension; Compensated advanced chronic liver disease; Dynamic changes; Liver decompensation; Liver stiffness measurement.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: The authors declare no competing interests. Ethical statement: All procedures followed were in accordance with the 1975 Helsinki Declaration, as revised in 2008. The study protocol was approved by the Ethics Committee of Beijing Ditan Hospital (approval number: DTEC-KY2024-069-01). Consent to participate: Informed consent was obtained from all individual participants included in the study.
Figures
Similar articles
-
Spleen stiffness measurement by vibration-controlled transient elastography at 100 Hz for non-invasive predicted diagnosis of clinically significant portal hypertension in patients with compensated advanced chronic liver disease: a modelling study.Lancet Gastroenterol Hepatol. 2024 Dec;9(12):1111-1120. doi: 10.1016/S2468-1253(24)00234-6. Epub 2024 Sep 23. Lancet Gastroenterol Hepatol. 2024. PMID: 39326431
-
Prognostic performance of non-invasive tests for portal hypertension is comparable to that of hepatic venous pressure gradient.J Hepatol. 2024 May;80(5):744-752. doi: 10.1016/j.jhep.2023.12.028. Epub 2024 Jan 11. J Hepatol. 2024. PMID: 38218352
-
Validation and expansion of Baveno VII criteria for cACLD and CSPH based on liver stiffness and platelet count: Correlation with risk of hepatic decompensation and death.Hepatology. 2025 Aug 1;82(2):422-437. doi: 10.1097/HEP.0000000000001183. Epub 2024 Dec 2. Hepatology. 2025. PMID: 39689352 Free PMC article.
-
Diagnostic accuracy of transient elastography in diagnosing clinically significant portal hypertension in patients with chronic liver disease: a systematic review and meta-analysis.J Med Ultrason (2001). 2022 Jul;49(3):333-346. doi: 10.1007/s10396-022-01239-x. Epub 2022 Jul 25. J Med Ultrason (2001). 2022. PMID: 35876975
-
Noninvasive liver disease assessment to identify portal hypertension: Systematic and narrative reviews supporting the AASLD Practice Guideline.Hepatology. 2025 Mar 1;81(3):1086-1104. doi: 10.1097/HEP.0000000000000841. Epub 2024 Mar 15. Hepatology. 2025. PMID: 38489516
References
-
- Shearer JE, Jones R, Parker R, et al. The natural history of advanced chronic liver disease defined by transient elastography. Clin Gastroenterol Hepatol. 2023. 10.1016/j.cgh.2022.03.015. - PubMed
-
- Segna D, Mendoza YP, Lange NF, et al. Non-invasive tools for compensated advanced chronic liver disease and portal hypertension after Baveno VII - an update. Dig Liver Dis. 2023;55(3):326–35. 10.1016/j.dld.2022.10.009. - PubMed
MeSH terms
Grants and funding
- 82474426/National Natural Science Foundation of China
- 82474419/National Natural Science Foundation of China
- 7232272/Beijing Municipal Natural Science Foundation
- zyyzdxk-2023005/high-level Chinese Medicine Key Discipline Construction Project
- 2024-1-2173/Capital's Funds for Health improvement and Research
LinkOut - more resources
Full Text Sources
Medical
