

Relative change rate of liver stiffness measurements predicts the risk of liver decompensation in compensated advanced chronic liver disease
- PMID: 40719905
- PMCID: PMC12304040
- DOI: 10.1007/s10238-025-01813-w
Relative change rate of liver stiffness measurements predicts the risk of liver decompensation in compensated advanced chronic liver disease
Abstract
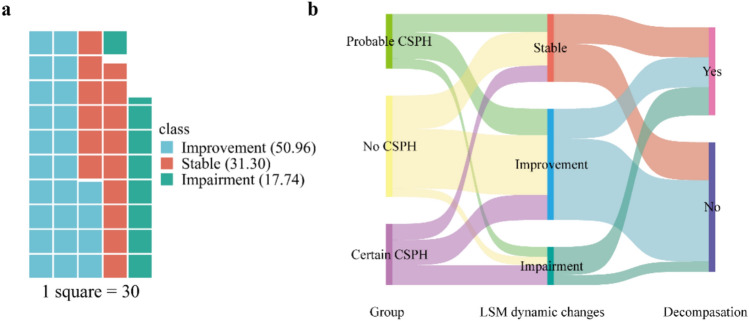
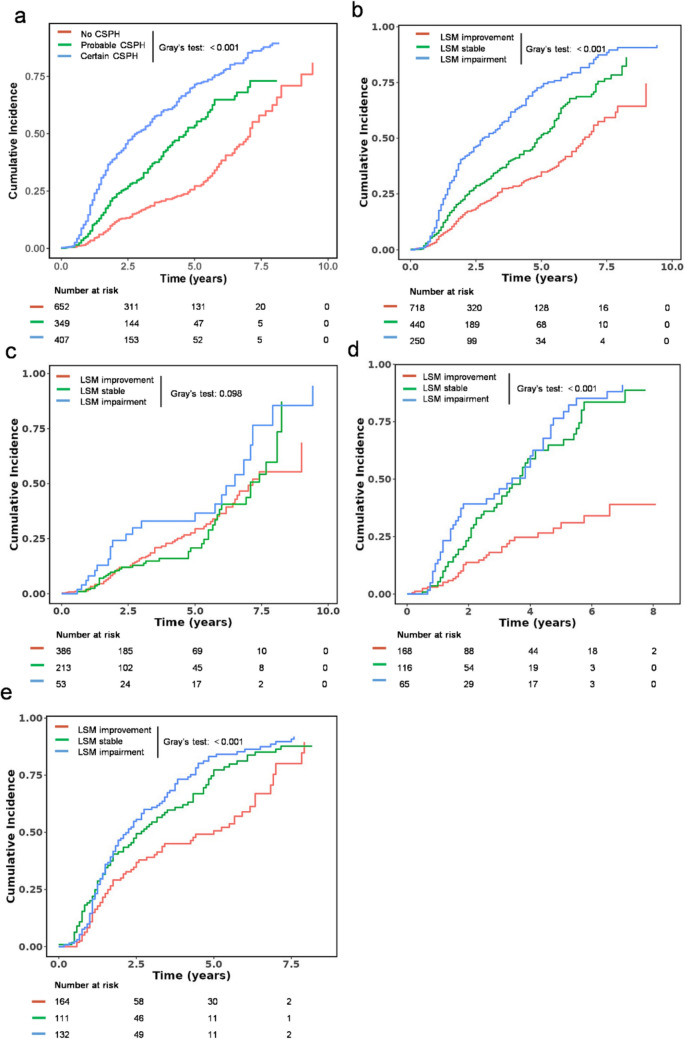
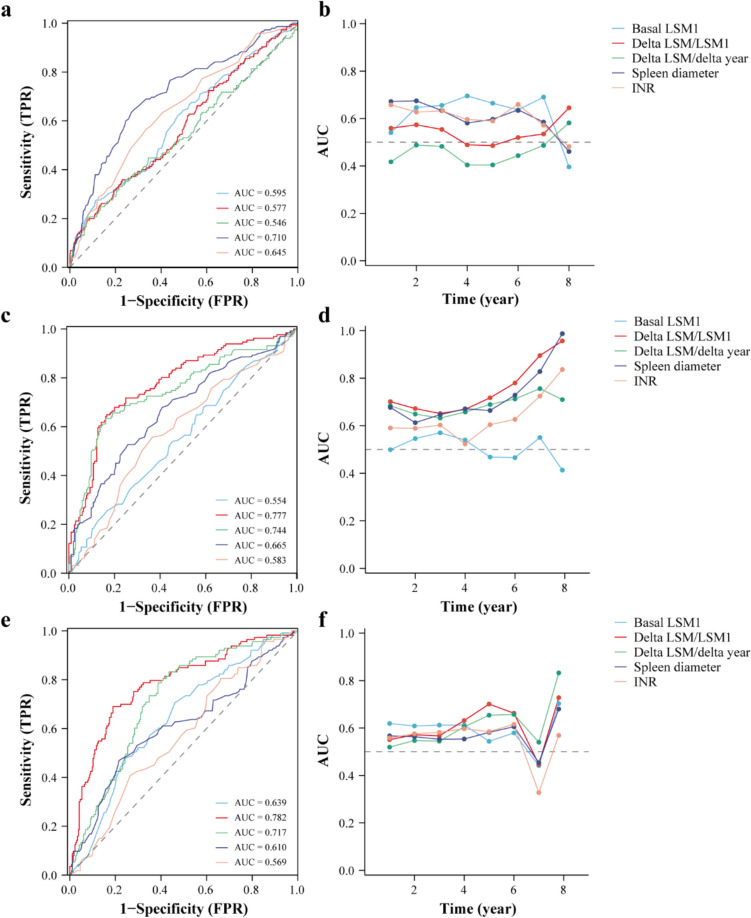
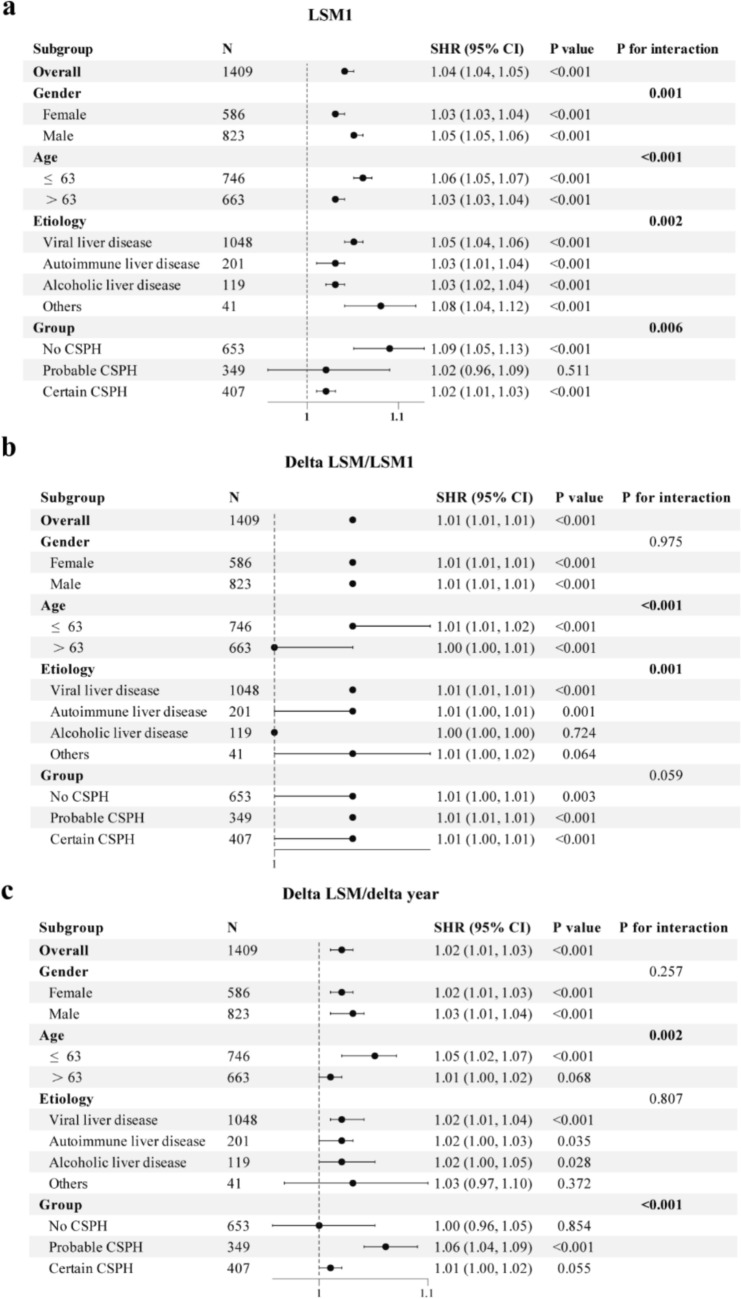
Patients with compensated advanced chronic liver disease (cACLD) have a significant risk of decompensation. Therefore, this study aimed to evaluate the predictive value of dynamic liver stiffness measurements (LSM) for decompensation risk, and their performance across different clinically significant portal hypertension (CSPH) risk stratification. This retrospective cohort study included 1409 patients with cACLD. Patients were divided into no CSPH, probable CSPH, and certain CSPH groups. Competing risk regression analysis was used to identify the independent predictors. The receiver operating characteristic curve and time-dependent area under the curve were used to evaluate the predictive performance. During follow-up, liver decompensation incidence increased with CSPH severity (22.2% with no CSPH, 37.5% with probable CSPH, and 64.9% with certain CSPH, p < 0.001). Multivariate regression analysis identified age, basal LSM1, delta LSM/LSM1, delta LSM/delta year, spleen diameter, and international normalized ratio as independent risk factors for liver decompensation. In the no CSPH group, spleen diameter showed the best predictive ability (AUC = 0.710). For probable and certain CSPH groups, delta LSM/LSM1 showed superior predictive performance (AUC: 0.777 and 0.782, respectively). The predictive power of basal LSM1 was relatively limited across all groups (AUC: 0.554-0.639). Subgroup analysis revealed interactions between age, sex, different etiologies, and CSPH subgroups. The relative change rate of LSM outperformed basal LSM1 and annual change rate in predicting liver decompensation risk, particularly in patients with existing portal hypertension. Dynamic assessments and differentiated prediction strategies are essential for optimal patient managements.
Keywords: Clinically significant portal hypertension; Compensated advanced chronic liver disease; Dynamic changes; Liver decompensation; Liver stiffness measurement.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: The authors declare no competing interests. Ethical statement: All procedures followed were in accordance with the 1975 Helsinki Declaration, as revised in 2008. The study protocol was approved by the Ethics Committee of Beijing Ditan Hospital (approval number: DTEC-KY2024-069-01). Consent to participate: Informed consent was obtained from all individual participants included in the study.
Figures
References
MeSH terms
Grants and funding
- 82474426/National Natural Science Foundation of China
- 82474419/National Natural Science Foundation of China
- 7232272/Beijing Municipal Natural Science Foundation
- zyyzdxk-2023005/high-level Chinese Medicine Key Discipline Construction Project
- 2024-1-2173/Capital's Funds for Health improvement and Research
LinkOut - more resources
Full Text Sources
Medical
