

Effect of foot reflexology on chronic pain in Parkinson's disease: A randomized controlled trial
- PMID: 40720491
- PMCID: PMC12303304
- DOI: 10.1371/journal.pone.0327865
Effect of foot reflexology on chronic pain in Parkinson's disease: A randomized controlled trial
Abstract
Objectives: Effectiveness of Foot Reflexology (FR) on the pain intensity in Parkinson's disease (PD) compared with Sham Massage (SM).
Design: Monocentric, longitudinal, prospective, double-blind, randomized controlled trial. Randomization with a random number generator in the R software. Fixed-sized block randomization of 3 implemented into Clinsight.
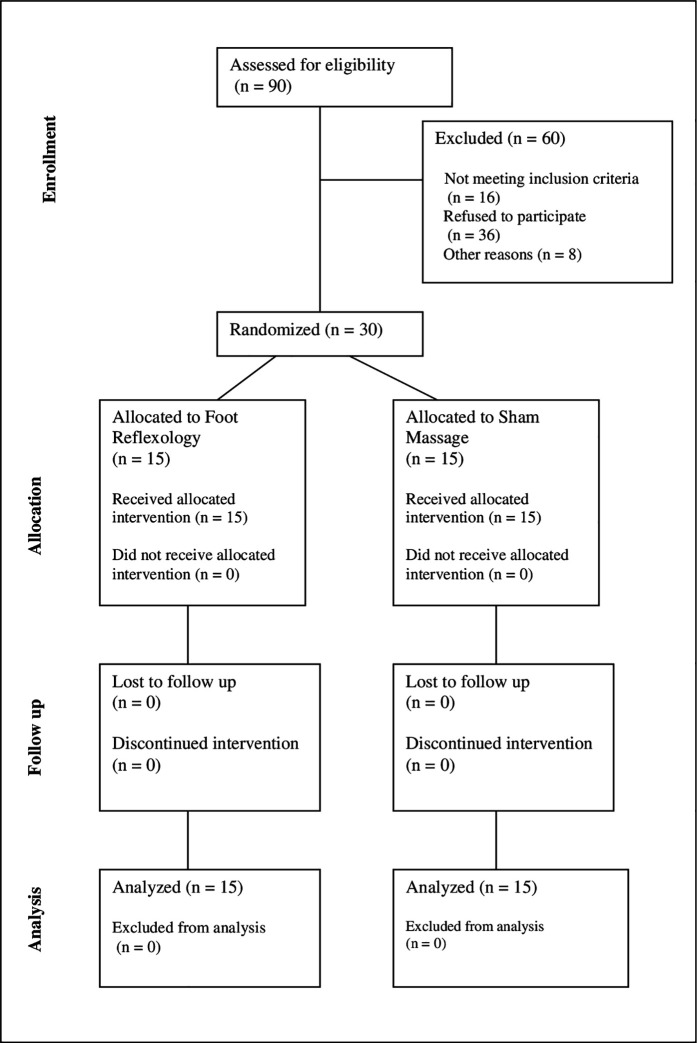
Participants: Idiopathic PD patients with chronic pain (Visual Analogue Scale (VAS)≥4) were recruited from the Toulouse University Hospital between the 14th of April 2021 and the 25th of May 2025.
Intervention: Four one-hour long FR or SM sessions three weeks apart with the same specialized FR researcher.
Main outcome measure: Pain intensity change measured by the mean VAS before and after full completed interventions. The difference was compared between group using a Wilcoxon Mann Witney test. Exploratory outcome: brain functional connectivity.
Results: 30 PD patients were randomized and analyzed. Interventions were delivered as planned for all patients. Clinical variables did not significantly differed between FR and SM groups. Mean VAS decreased by -12.3 mm ± 15.2 in FR group (n = 15) and -17.9 mm ± 29.4 in SM group (n = 15). Analyses did not reveal any significant difference between the FR and SM groups (p-value = 0.88). There are different patterns in connectivity changes in the medial pain system between responders (at least 30% pain reduction) and non-responders to both therapies. There were no adverse events.
Conclusion: FR is not more effective than SM in relieving chronic pain in PD. The differences in connectivity patterns within the medial pain pathway may underlie the response to tactile stimulation (FR and SM).
Trial registration: ClinicalTrials.gov NCT04705207.
Copyright: © 2025 Joineau et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
There is no conflicts of interests relevant to this work. Financial Disclosures for the previous 12 months: KJ has nothing to declare. EH received support for attending meetings and/or travel from NHC. MB has nothing to declare. MF declares honoraria from LVL Medical, BIAL, AbbVie, and Orkyn for speaking and from consultancy work unrelated to this research. CL received support for attending meetings and/or travel from AbbVie, Elivie, Mertz, Ipsen, Medtronic, Orkyn, and NHC unrelated to this research. FOM served on boards for AbbVie, Aguettant, Elivie, and Orphalan and carried out consulting activities for Aguettant, Abbvie, Orkyn, and NHC. She received travel grants from AbbVie, all of which were unrelated to this research. VR has nothing to declare. PP has nothing to declare. CBC received a research grant from France Parkinson and fees for lectures and consultancy work for Aguettant, Orkyn, Zambon, NHC, and AbbVie, all of which were unrelated to this research. ED has nothing to declare.
Figures

References
-
- Negre-Pages L. Douleur et anxiété dans la maladie de Parkinson. Université de Toulouse, Université Toulouse III - Paul Sabatier. 2008. http://thesesups.ups-tlse.fr/367/
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
