

Concomitant Surgical Ablation in Atrial Fibrillation Patients Undergoing Cardiac Surgery for Isolated Coronary and Aortic Valve Disease: A Multicentre Study from The Netherlands Heart Registration
- PMID: 40720587
- PMCID: PMC12342894
- DOI: 10.1093/ejcts/ezaf244
Concomitant Surgical Ablation in Atrial Fibrillation Patients Undergoing Cardiac Surgery for Isolated Coronary and Aortic Valve Disease: A Multicentre Study from The Netherlands Heart Registration
Abstract
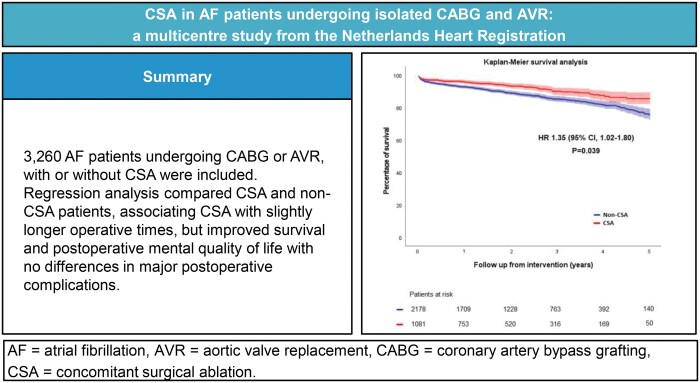
Objectives: Concomitant surgical ablation (CSA) is recommended for atrial fibrillation (AF) patients undergoing cardiac surgery; however, its effects in non-mitral valve surgeries, specifically coronary artery bypass grafting (CABG) and aortic valve replacement (AVR), are less studied. This study aims to analyse outcomes and trends of CSA performance in the Netherlands.
Methods: This nationwide multicentre study utilized data from the Netherlands Heart Registration. AF patients undergoing CABG or AVR between 2013 and 2021 were included. Temporal trends in CSA performance were analysed and a multivariable regression model adjusted for confounders when comparing CSA and non-CSA.
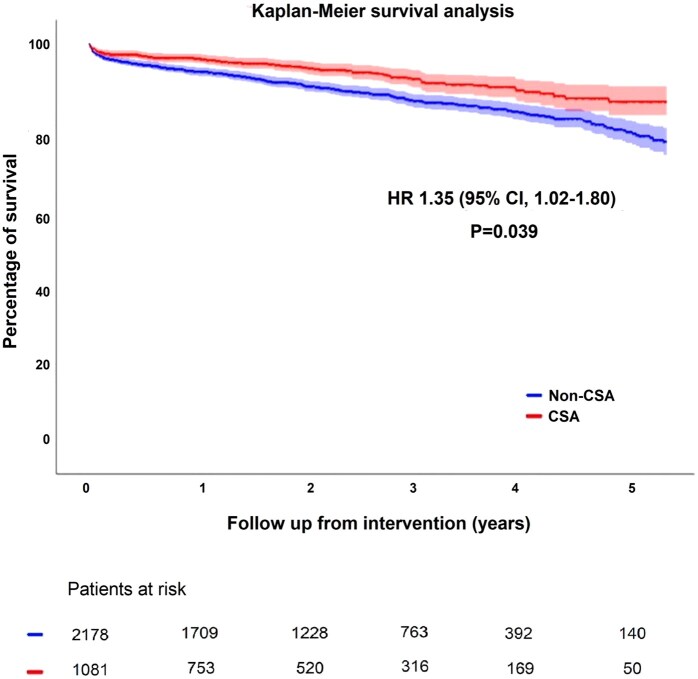
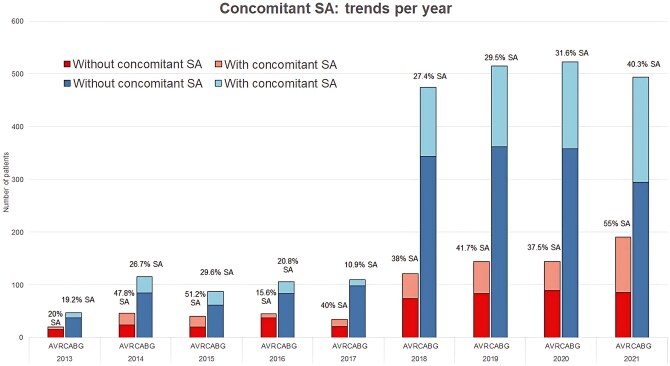
Results: A total of 3260 patients were included, of which 1081 underwent CSA. CSA patients showed longer cardiopulmonary bypass (CPB) (111 vs 80, mean difference between groups: 31 min [95% CI, 27-34, P < 0.001]) and aortic cross clamping (AoX) times (67 vs 52, mean difference: 15 min [95% CI, 13-17, P < 0.001]). After correcting for confounders, CSA patients presented mean CPB and AoX times of 18 (95% CI, 16-21, P < 0.001) and 8 (95% CI, 6-10, P < 0.001) min longer. The CSA group showed higher survival rates (92.5% vs 86.4%, P = 0.039) and greater improvements in mental quality of life (QoL) (P = 0.047). CSA performance during CABG and AVR has increased significantly, from 29.7% in 2018 to 44.4% in 2021.
Conclusions: CSA resulted in slightly longer CPB and AoX times but no significant differences in major complications. Regression analysis showed better survival rates and improved mental QoL for CSA. CSA performance in CABG and AVR has increased in the Netherlands.
Keywords: aortic valve replacement; atrial fibrillation; concomitant surgical ablation; coronary artery bypass grafting.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Conflict of interest statement
None declared.
Figures

References
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023;147:e93-e621. - PMC - PubMed
-
- Van Gelder IC, Rienstra M, Bunting KV, et al. ESC guidelines for the management of atrial fibrillation. Eur Heart J. 2024;45:ehae176.
-
- Badhwar V, Rankin JS, Ad N, et al. Surgical ablation of atrial fibrillation in the United States: trends and propensity matched outcomes. Ann Thorac Surg. 2017;104:493-500. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
