

Features, Outcome, and Treatment of Postanoxic Status Epilepticus: Pooled Analysis of 3 Cohorts
- PMID: 40720710
- PMCID: PMC12296630
- DOI: 10.1212/WNL.0000000000213913
Features, Outcome, and Treatment of Postanoxic Status Epilepticus: Pooled Analysis of 3 Cohorts
Erratum in
-
Features, Outcome, and Treatment of Postanoxic Status Epilepticus: Pooled Analysis of 3 Cohorts.Neurology. 2025 Oct 21;105(8):e214282. doi: 10.1212/WNL.0000000000214282. Epub 2025 Sep 22. Neurology. 2025. PMID: 40982774 Free PMC article. No abstract available.
Abstract
Background and objectives: The prognostic significance and the benefits of antiseizure treatment for definite and possible status epilepticus (SE) after cardiac arrest (CA) remain debated. The study aims to identify clinical and EEG predictors of outcome in definite and possible SE after CA and to determine patient categories in which antiseizure medication is useful.
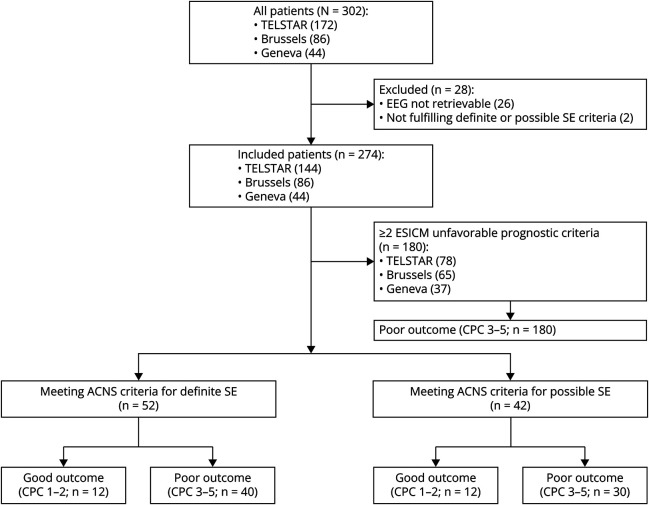
Methods: We conducted a multicenter pooled analysis of individual patient data from the Treatment of ELectroencephalographic STatus epilepticus After cardiopulmonary Resuscitation trial and 2 local registries (Brussels and Geneva). Patients with EEG patterns fulfilling the American Clinical Neurophysiology Society criteria for definite or possible SE within 72 hours after CA were included. Primary outcome was the cerebral performance category (CPC) at 3 months, dichotomized as good (CPC 1-2) or poor (CPC 3-5). Patients, clinical, EEG, and treatment characteristics were related to outcome using univariate and multivariate analyses in the whole cohort and separate for patients without ≥2 poor outcome European Resuscitation Council (ERC)/European Society of Intensive Care Medicine (ESICM) criteria. This latter group of patients was further divided into 2 subgroups: those with definite SE and those with possible SE.
Results: Of 274 patients (median age 66 [interquartile range (IQR) 55-75], 31% female) with definite or possible SE, 24 (8.8%) had good recovery. In multivariate analysis, nonmotor semiology and SE cessation were associated with good recovery. After exclusion of patients with ≥2 poor outcome ERC/ESICM criteria (180 patients), we included 94 patients (52 definite SE and 42 possible SE), 25% having good outcome. In definite SE, SE cessation (12 [100%] vs 20 [50%], p = 0.002), higher discharge frequency (3 Hz [IQR 2-3] vs 2 Hz [IQR 2-3], p = 0.024), guideline-recommended SE treatment (12 [100%] vs 28 [70%], p = 0.047), and higher doses of levetiracetam (4,250 [IQR 3,750-4,500] mg vs 2,000 [IQR 2,000-3,000] mg, p = 0.001) and valproic acid (4,800 [IQR 3,600-5,400] mg vs 2,000 [IQR 1,850-2,250] mg, p = 0.032) were associated with favorable outcome. None of the definite or possible SE patients with good outcome had a suppressed/suppression-burst background before SE onset.
Discussion: Patients with postanoxic definite or possible SE have a 25% chance of good outcome in the absence of ≥2 poor outcome ERC/ESICM factors. EEG background continuity before SE onset and higher discharge frequency contribute to the identification of patients who may benefit from protracted treatment.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical