

Beyond the triad: akinetic mutism in idiopathic normal pressure hydrocephalus, with response to shunt placement. Illustrative case
- PMID: 40720908
- PMCID: PMC12305355
- DOI: 10.3171/CASE25257
Beyond the triad: akinetic mutism in idiopathic normal pressure hydrocephalus, with response to shunt placement. Illustrative case
Abstract
Background: Idiopathic normal pressure hydrocephalus (iNPH) typically manifests with the classic Hakim-Adams triad of gait disturbance, cognitive impairment, and urinary incontinence. While akinetic mutism represents a rare and severe neurological presentation characterized by profound reduction in voluntary movement and speech, its association with iNPH remains underrecognized in clinical practice. This case illustrates both the diagnostic challenges and remarkable therapeutic potential when encountering this unusual manifestation of iNPH.
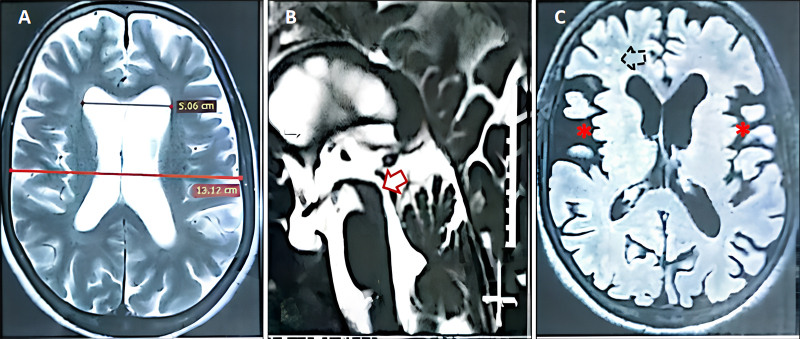
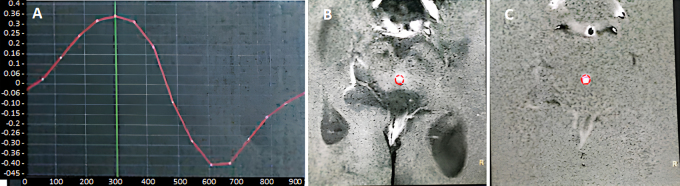
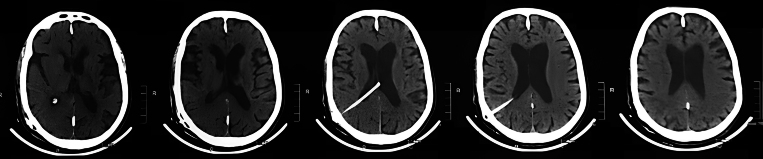
Observations: A previously healthy 52-year-old female developed progressive gait instability, urinary incontinence, and cognitive decline over 6 months, followed by 3 months of akinetic mutism. Examination demonstrated characteristic features of iNPH including paratonic rigidity, magnetic gait, and frontal release signs. Neuroimaging revealed moderate ventriculomegaly with an Evans index of 0.38 and hyperdynamic CSF flow dynamics (peak velocity 7.4 cm/sec, stroke volume 95 µL). The patient exhibited dramatic clinical improvement within 1 week of ventriculoperitoneal shunt placement, with complete resolution of akinetic mutism and significant recovery of other symptoms sustained at the 6-month follow-up.
Lessons: This case underscores that akinetic mutism, while uncommon, may represent a severe but treatable manifestation of iNPH. The rapid reversal of akinetic mutism following CSF diversion highlights the importance of considering iNPH even in atypical presentations. Quantitative CSF flow analysis emerges as a valuable diagnostic tool in such challenging cases, while the striking clinical response reinforces the potential for complete functional recovery with timely intervention. https://thejns.org/doi/10.3171/CASE25257.
Keywords: akinetic mutism; cerebrospinal fluid dynamics; hydrocephalus biomarkers; idiopathic normal pressure hydrocephalus; reversible dementia; ventriculoperitoneal shunt.
Figures
References
-
- Relkin N Marmarou A Klinge P Bergsneider M Black PM.. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005;57(3suppl):S2-S16. - PubMed
-
- Mori E, Ishikawa M, Kato T.Guidelines for management of idiopathic normal pressure hydrocephalus: second edition. Neurol Med Chir (Tokyo). 2nd ed. 2012;52(11):775-809. - PubMed
-
- Boon AJ, Tans JT, Delwel EJ.Dutch normal pressure hydrocephalus study: baseline characteristics with emphasis on clinical findings. Eur J Neurol. 1997;4(1):39-47. - PubMed
-
- Krauss JK Regel JP Droste DW Orszagh M Borremans JJ Vach W.. Movement disorders in adult hydrocephalus. Mov Disord. 1997;12(1):53-60. - PubMed
-
- Yamada S, Ishikawa M, Ito H.Cerebrospinal fluid dynamics in idiopathic normal pressure hydrocephalus on four-dimensional flow imaging. Eur Radiol. 2020;30(8):4454-4465. - PubMed
LinkOut - more resources
Full Text Sources
