

Rituximab induced lung injury
- PMID: 40722009
- PMCID: PMC12302443
- DOI: 10.1186/s12890-025-03802-x
Rituximab induced lung injury
Abstract
Background: Rituximab is a chimeric human-mouse immunoglobulin monoclonal antibody with high affinity for CD20 surface antigens expressed by pre-B and B cells that is commonly used as the mainstay for the treatment of B cell non-Hodgkin's lymphomas, including diffuse large B-cell lymphoma (DLBCL). As the drug has become more widely used, rituximab associated Interstitial Lung disease (RTX-ILD) is being recognized as potential complication (Non-infectious pulmonary toxicity of rituximab: a systematic review| Rheumatology| Oxford Academic).
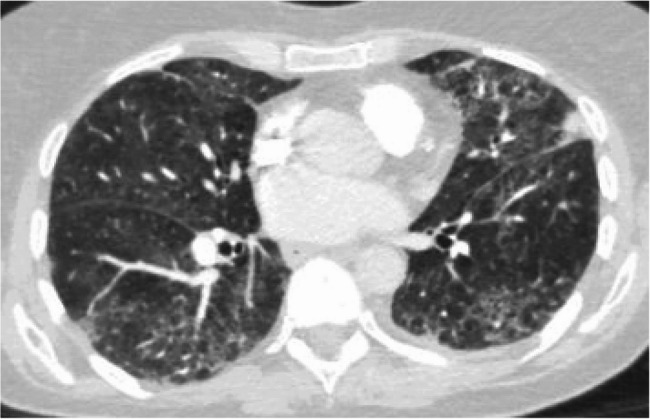
Case report: We discuss a 73-year-old woman with newly diagnosed DLBCL who underwent chemotherapy and immunotherapy with rituximab, cyclophosphamide, doxorubicin hydrochloride, vincristine sulphate, and prednisone (R-CHOP). Following her initial rituximab infusion, she developed shortness of breath, chills, rigors, flushing, and agitation. The rituximab infusion was paused, and hypersensitivity reaction medications were given per protocol. The infusion was resumed at a slower rate. Two weeks after initial infusion, she was hospitalized for shortness of breath and hypoxemia to 88% on pulse oximeter requiring 2 L of nasal cannula oxygen. Chest imaging showed new diffuse ground glass opacities (GGOs) on top of apical scarring, upper lobe emphysema, and few calcified granulomas. Patient underwent bronchoscopy for bronchoalveolar lavage (BAL) which was negative for infections and malignancy. Given the temporal relationship, chemotherapy induced lung injury was high on the differential, with rituximab being the possible offending agent. She was started on prednisone 60 milligram for 5 days with a follow up chest imaging showing resolution of the acute GGO. Her O2 requirements decreased from 3 L to 1 L and she was sent home with oxygen. Given the curative intent of R-CHOP, after shared decision making with the patient and her medical team, a treatment plan with a longer course of high and low prednisone was incorporated as part of her chemotherapy session. She was able to successfully finish her treatment with no additional episode, at which point she was able to be successfully tapered off her prednisone.
Discussion: Rituximab induced ILD is rare but given its severity requires a high index of suspicion for diagnosis. Given the potential for long term complication, once suspected, treatment should be discontinued. Here we detail how a prolonged steroid course could be used as adjunct therapy of ILD if therapy with rituximab is considered curative and essential.
Conclusion: Rituximab and Cyclophosphamide are well described causes of acute pneumonitis post R-CHOP administration. Given curative effect of R-CHOP, careful changes in management plan and co-treatment with steroids could help preserve lung function while allowing for full continuation of the chemotherapy regimen.
Keywords: Chemotherapy toxicity; Interstitial lung disease; Rituximab.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Verbal consent obtained from the patient. Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient’s spouse. A copy of the consent form is available for review by the Editor of this journal. Competing interests: The authors declare no competing interests.
Figures

References
-
- Non-infectious pulmonary toxicity of rituximab: a systematic review| Rheumatology| Oxford Academic. Accessed April 11. 2024. https://academic.oup.com/rheumatology/article/51/4/653/1802004?login=false. - PubMed
-
- Friedberg JW. Unique toxicities and resistance mechanisms associated with monoclonal antibody therapy. Hematol Am Soc Hematol Educ Program Published Online 2005:329–34. 10.1182/asheducation-2005.1.329. - PubMed
-
- Boffetta PI. Epidemiology of adult non-Hodgkin lymphoma. Ann Oncol. 2011;22:iv27–31. 10.1093/annonc/mdr167.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
