

Evaluation of the impact of artificial intelligence-assisted image interpretation on the diagnostic performance of clinicians in identifying endotracheal tube position on plain chest X-ray: a multi-case multi-reader study
- PMID: 40722100
- PMCID: PMC12305994
- DOI: 10.1186/s13054-025-05566-6
Evaluation of the impact of artificial intelligence-assisted image interpretation on the diagnostic performance of clinicians in identifying endotracheal tube position on plain chest X-ray: a multi-case multi-reader study
Abstract
Background: Incorrectly placed endotracheal tubes (ETTs) can lead to serious clinical harm. Studies have demonstrated the potential for artificial intelligence (AI)-led algorithms to detect ETT placement on chest X-Ray (CXR) images, however their effect on clinician accuracy remains unexplored. This study measured the impact of an AI-assisted ETT detection algorithm on the ability of clinical staff to correctly identify ETT misplacement on CXR images.
Methods: Four hundred CXRs of intubated adult patients were retrospectively sourced from the John Radcliffe Hospital (Oxford) and two other UK NHS hospitals. Images were de-identified and selected from a range of clinical settings, including the intensive care unit (ICU) and emergency department (ED). Each image was independently reported by a panel of thoracic radiologists, whose consensus classification of ETT placement (correct, too low [distal], or too high [proximal]) served as the reference standard for the study. Correct ETT position was defined as the tip located 3-7 cm above the carina, in line with established guidelines. Eighteen clinical readers of varying seniority from six clinical specialties were recruited across four NHS hospitals. Readers viewed the dataset using an online platform and recorded a blinded classification of ETT position for each image. After a four-week washout period, this was repeated with assistance from an AI-assisted image interpretation tool. Reader accuracy, reported confidence, and timings were measured during each study phase.
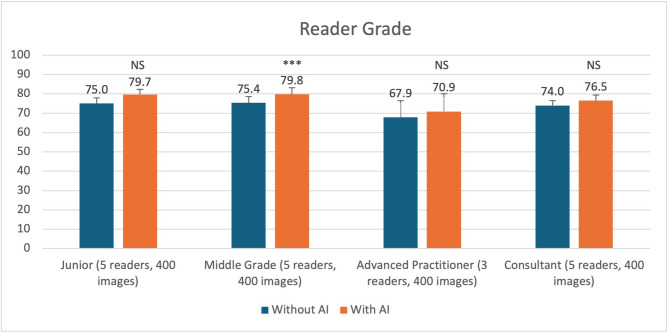
Results: 14,400 image interpretations were undertaken. Pooled accuracy for tube placement classification improved from 73.6 to 77.4% (p = 0.002). Accuracy for identification of critically misplaced tubes increased from 79.3 to 89.0% (p = 0.001). Reader confidence improved with AI assistance, with no change in mean interpretation time at 36 s per image.
Conclusion: Use of assistive AI technology improved accuracy and confidence in interpreting ETT placement on CXR, especially for identification of critically misplaced tubes. AI assistance may potentially provide a useful adjunct to support clinicians in identifying misplaced ETTs on CXR.
Keywords: Artificial intelligence; Chest X-ray; Endotracheal tube; Medical imaging; Radiology; Tube misplacement.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All participants provided written informed consent before enrolment in the study. The consent process included a detailed explanation of the study’s purpose, procedures, potential risks and benefits, and the voluntary nature of participation. Participants were informed about the two phases of the study - interpreting chest X-rays without and then with AI assistance after a washout period. They were made aware that their interpretations would be compared to expert radiologist readings. Participants were assured of their right to withdraw from the study at any time without any negative consequences. Participants were also informed that their anonymised data would be analysed and potentially published in aggregate form. The consent process emphasized that participation was voluntary and would not affect their employment or standing at their institution. Consent for publication: Not Applicable. This manuscript does not contain any individual person’s data in any form, including identifying images or personal or clinical details that could compromise anonymity. As such, no specific consent for publication was required from any individuals. All data presented in this study are aggregated and anonymized, ensuring the privacy and confidentiality of all participants involved in the research. We have adhered strictly to ethical guidelines and data protection regulations throughout the study and in the preparation of this manuscript. Competing interests: AS, SG, AB are employed by GE HealthCare, a key NCIMI stakeholder. AN and CB have undertaken paid consultancy work for GEHC. PA, SA and FG are employees of Report and Image Quality Control (http://www.raiqc.com RAIQC), a spin-out company from Oxford University Hospitals NHS Foundation Trust. A.Shah is an Editor of Anaesthesia and has received honorariums from Pharmacosmos UK, outside of the submitted work. JSB is a Senior Clinical Advisor to Intelligent Ultrasound, a company making AI products for medical ultrasound. There are no other relationships or activities that could appear to have influenced the submitted work.
Figures




References
-
- Özkurtul O, Struck MF, Fakler J, Bernhard M, Seinen S, Wrigge H, et al. Physician-based on-scene airway management in severely injured patients and in-hospital consequences: is the misplaced intubation an underestimated danger in trauma management? Trauma Surg Acute Care Open. 2019;4(1):e000271. - PMC - PubMed
-
- Jemmett ME, Kendal KM, Fourre MW, Burton JH. Unrecognized misplacement of endotracheal tubes in a mixed urban to rural emergency medical services setting. Acad Emerg Med. 2003;10(9):961–5. - PubMed
-
- Maybauer D, Maybauer M, Wolff H, Pfenninger E, Geisser W. Radiological validation of endotracheal tube insertion depth in prehospital emergency patients. Crit Care. 2009;13(Suppl 1):P3. - PubMed
-
- Wang HE, Cook LJ, Chang CCH, Yealy DM, Lave JR. Outcomes after out-of-hospital endotracheal intubation errors. Resuscitation. 2009;80(1):50–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
