

Obstructive Sleep Apnea and Outcomes in Cardiac Surgery: A Systematic Review with Meta-Analytic Synthesis (PROSPERO CRD420251049574)
- PMID: 40722654
- PMCID: PMC12292749
- DOI: 10.3390/biomedicines13071579
Obstructive Sleep Apnea and Outcomes in Cardiac Surgery: A Systematic Review with Meta-Analytic Synthesis (PROSPERO CRD420251049574)
Abstract
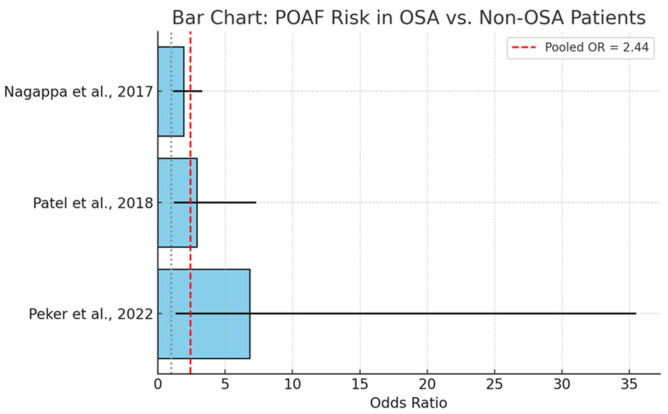
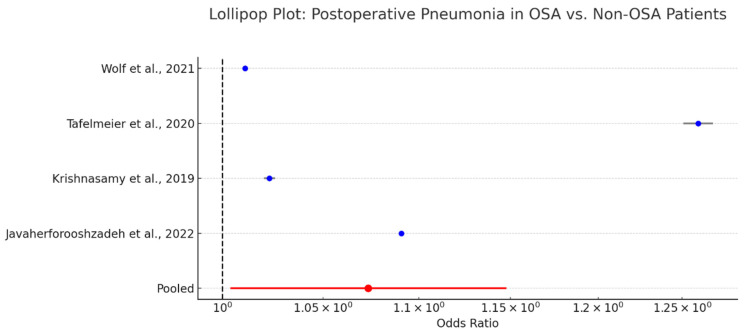
Background: Obstructive sleep apnea (OSA) is a prevalent but frequently underdiagnosed comorbidity in patients undergoing cardiac surgery, including coronary artery bypass grafting (CABG), aortic valve replacement (AVR), and mitral valve repair or replacement (MVR). This systematic review and meta-analytic synthesis investigates the relationship between OSA and postoperative morbidity and mortality, with particular attention to the predictive utility of established screening instruments. Methods: A systematic search of the PubMed database was conducted (April 2025), identifying 724 articles published in the last ten years. Seventeen primary studies met the inclusion criteria for qualitative synthesis, and four additional studies were included in the meta-analyses. Outcomes assessed included atrial fibrillation, major adverse cardiac and cerebrovascular events (MACCE), acute kidney injury (AKI), respiratory complications, pneumonia, hospital length of stay (LOS), and mortality. Risk of bias was assessed qualitatively based on study design and reporting limitations. This review was registered in the PROSPERO database under registration number CRD420251049574. Results: Meta-analyses demonstrated significantly elevated odds of atrial fibrillation (OR = 2.44, 95% CI: 1.46-4.07), major adverse cardiac and cerebrovascular events (OR = 2.06, 95% CI: 1.61-2.63), acute kidney injury (OR = 2.24, 95% CI: 1.67-3.01), and respiratory complications (OR = 1.15, 95% CI: 1.05-1.25) among patients with OSA. Additionally, OSA was associated with a significantly prolonged hospital length of stay (standardized mean difference [SMD] = 0.62, 95% CI: 0.46-0.78) and a marginal increase in pneumonia risk (OR = 1.07, 95% CI: 1.00-1.15). Evidence regarding stroke, intensive care unit (ICU) stay, and mortality was inconsistent or underpowered. Conclusions: Across core outcomes, findings were consistent across multiple studies involving a large patient population. Obstructive sleep apnea is a clinically consequential risk factor in cardiac surgery, associated with increased perioperative complications and prolonged hospitalization. These findings support the integration of routine OSA screening into preoperative risk assessment protocols. Further prospective, multicenter trials are warranted to assess the efficacy of perioperative management strategies, including continuous positive airway pressure (CPAP) therapy, in improving surgical outcomes.
Keywords: CPAP; MACCE; atrial fibrillation; cardiac surgery; meta-analysis; obstructive sleep apnea; postoperative complications; risk stratification.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures










Similar articles
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Limited versus full sternotomy for aortic valve replacement.Cochrane Database Syst Rev. 2017 Apr 10;4(4):CD011793. doi: 10.1002/14651858.CD011793.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2023 Dec 6;12:CD011793. doi: 10.1002/14651858.CD011793.pub3. PMID: 28394022 Free PMC article. Updated.
-
The effectiveness of positive airway pressure therapy in reducing postoperative adverse outcomes in surgical patients with obstructive sleep apnea: A systematic review and meta-analysis.J Clin Anesth. 2023 Feb;84:110993. doi: 10.1016/j.jclinane.2022.110993. Epub 2022 Nov 5. J Clin Anesth. 2023. PMID: 36347195
-
Continuous positive airway pressure (CPAP) during the postoperative period for prevention of postoperative morbidity and mortality following major abdominal surgery.Cochrane Database Syst Rev. 2014 Aug 1;2014(8):CD008930. doi: 10.1002/14651858.CD008930.pub2. Cochrane Database Syst Rev. 2014. PMID: 25081420 Free PMC article.
-
Postoperative Outcomes in Obstructive Sleep Apnea Patients Undergoing Cardiac Surgery: A Systematic Review and Meta-analysis of Comparative Studies.Anesth Analg. 2017 Dec;125(6):2030-2037. doi: 10.1213/ANE.0000000000002558. Anesth Analg. 2017. PMID: 29049073
References
-
- Yeghiazarians Y., Jneid H., Tietjens J.R., Redline S., Brown D.L., El-Sherif N., Mehra R., Bozkurt B., Ndumele C.E., Somers V.K. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation. 2021;144:E56–E67. doi: 10.1161/CIR.0000000000000988. - DOI - PubMed
-
- Maniaci A., Lavalle S., Parisi F.M., Barbanti M., Cocuzza S., Iannella G., Magliulo G., Pace A., Lentini M., Masiello E., et al. Impact of Obstructive Sleep Apnea and Sympathetic Nervous System on Cardiac Health: A Comprehensive Review. J. Cardiovasc. Dev. Dis. 2024;11:204. doi: 10.3390/jcdd11070204. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
