

Cumulative Transcutaneous Spinal Stimulation with Locomotor Training Safely Improves Trunk Control in Children with Spinal Cord Injury: Pilot Study
- PMID: 40723009
- PMCID: PMC12293838
- DOI: 10.3390/children12070817
Cumulative Transcutaneous Spinal Stimulation with Locomotor Training Safely Improves Trunk Control in Children with Spinal Cord Injury: Pilot Study
Abstract
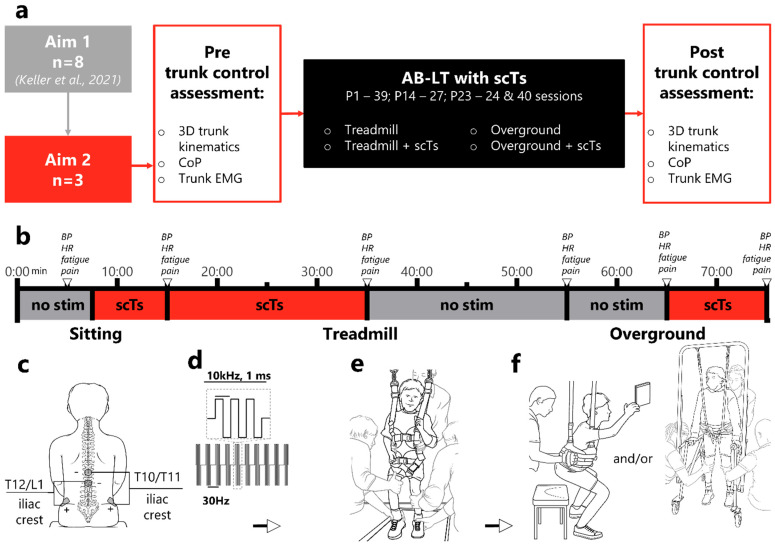
Background/objectives: Non-invasive spinal cord transcutaneous stimulation (scTS) has expanded the therapeutic landscape of spinal cord injury (SCI) rehabilitation, offering potential benefits beyond compensatory approaches to paralysis. Children with SCI are particularly susceptible to developing neuromuscular scoliosis due to trunk muscle paralysis and ongoing skeletal growth, making targeted interventions crucial. As demonstrated in adults and pediatrics with SCI, the ability of scTS to acutely and safely enable an upright posture and trunk control could be leveraged as a therapeutic adjunct. Activity-based locomotor training (AB-LT) alone significantly improves trunk control in children with SCIs; combining it with scTS may enhance outcomes. This pilot study evaluated the safety, feasibility, and cumulative effects of AB-LT combined with scTS on trunk control in children with SCI.
Methods: Three children with SCI completed 19 to 64 sessions of combined AB-LT and scTS. Adverse effects were monitored session to session, and trunk control was assessed pre- and post-intervention.
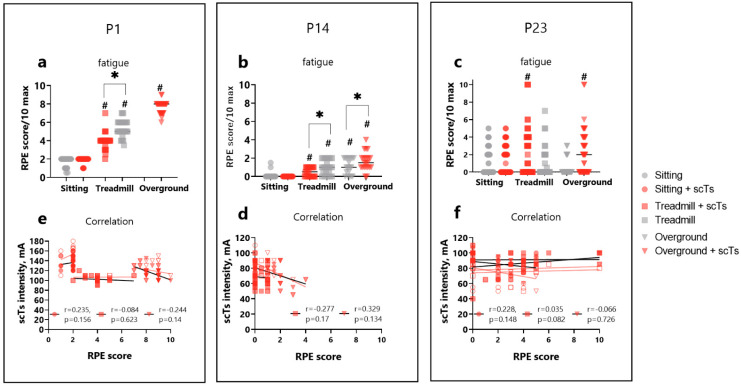
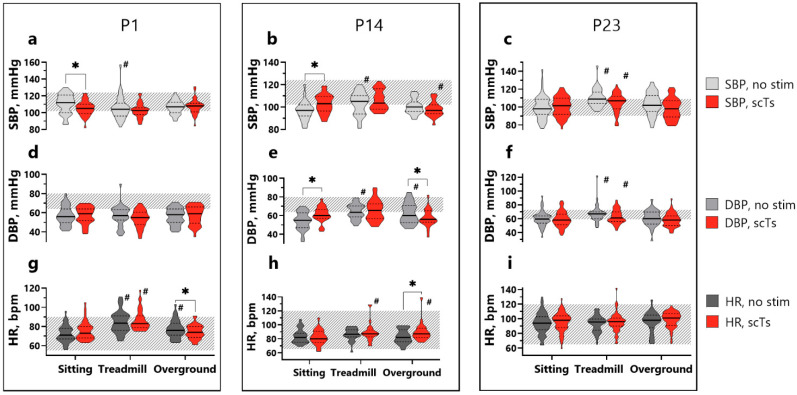
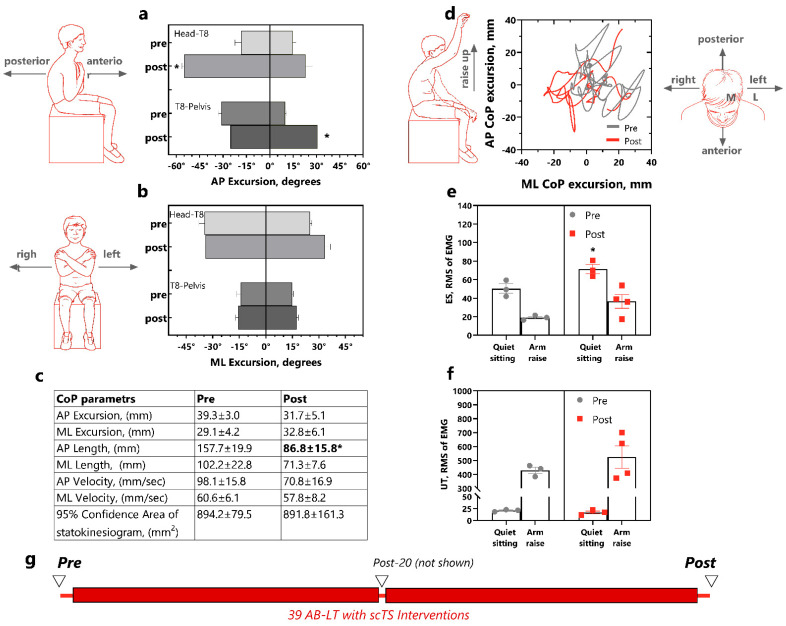
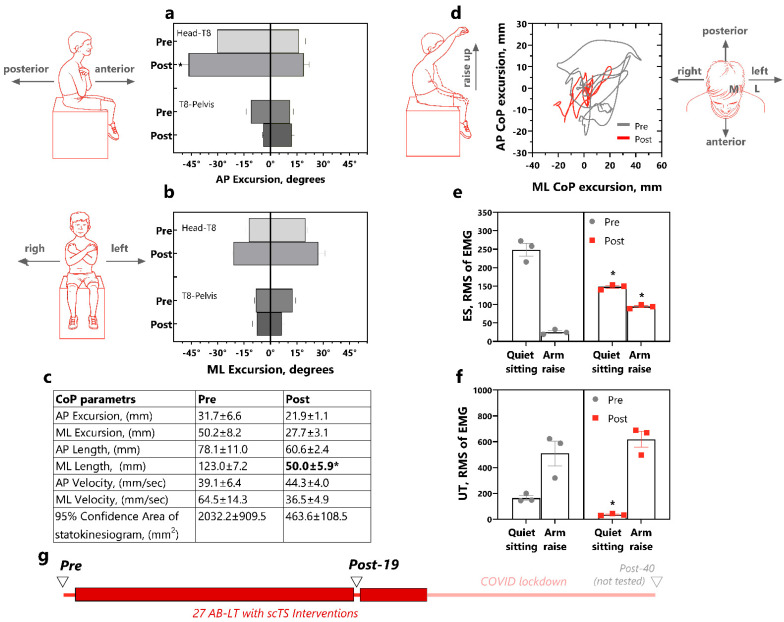
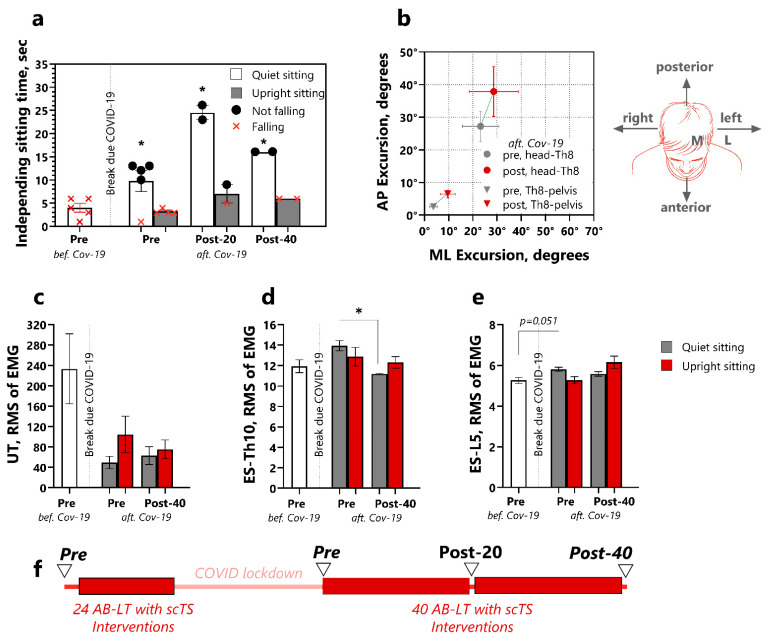
Results: Across 130 interventions in three participants, 88.5% of sessions were free from adverse effects. Reported adverse events included autonomic dysreflexia (5.4%), skin redness at electrode sites (4.6%), and headaches (1.5%). No significant impact of scTS on fatigue or central hemodynamic parameters was observed. Post-intervention, all participants demonstrated improved trunk control during quiet and perturbed sitting.
Conclusions: These findings provide the first evidence supporting the safety and feasibility of this combinatorial approach in pediatric SCI rehabilitation while emphasizing the importance of monitoring skin integrity and signs of autonomic dysreflexia. This intervention shows potential synergistic benefits, warranting further research to confirm efficacy and optimize therapeutic protocols.
Keywords: activity-based locomotor training; pediatrics; spinal cord injury; spinal cord transcutaneous stimulation; trunk control.
Conflict of interest statement
Yury Gerasimenko has a shareholder interest in NeuroRecovery Technologies and Cosyma. He holds certain inventorship rights on intellectual property licensed by the regents of the University of California to NeuroRecovery Technologies and its subsidiaries. The University of Louisville holds the licenses for the medical devices: pediatric treadmill/body weight support system and harnesses with Andrea Behrman as a co-inventor. Behrman is a volunteer, President of NeuroRecovery Learning, Inc. providing on-line and live course in activity-based locomotor training, as well as co-author of the book, Locomotor Training: Principles and Practice, 2011. Liubov Amirova, Anastasia Keller, Goutam Singh, Molly King, Parth Parikh, Nicole Stepp, and Beatrice Ugiliweneza declare no conflict of interest.
Figures
Similar articles
-
Technological aids for the rehabilitation of memory and executive functioning in children and adolescents with acquired brain injury.Cochrane Database Syst Rev. 2016 Jul 1;7(7):CD011020. doi: 10.1002/14651858.CD011020.pub2. Cochrane Database Syst Rev. 2016. PMID: 27364851 Free PMC article.
-
Physical exercise training interventions for children and young adults during and after treatment for childhood cancer.Cochrane Database Syst Rev. 2013 Apr 30;(4):CD008796. doi: 10.1002/14651858.CD008796.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2016 Mar 31;3:CD008796. doi: 10.1002/14651858.CD008796.pub3. PMID: 23633361 Updated.
-
Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews.Cochrane Database Syst Rev. 2017 Apr 24;4(4):CD011279. doi: 10.1002/14651858.CD011279.pub3. Cochrane Database Syst Rev. 2017. PMID: 28436583 Free PMC article.
-
Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews.Cochrane Database Syst Rev. 2017 Jan 14;1(1):CD011279. doi: 10.1002/14651858.CD011279.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2017 Apr 24;4:CD011279. doi: 10.1002/14651858.CD011279.pub3. PMID: 28087891 Free PMC article. Updated.
-
Physical exercise training interventions for children and young adults during and after treatment for childhood cancer.Cochrane Database Syst Rev. 2016 Mar 31;3(3):CD008796. doi: 10.1002/14651858.CD008796.pub3. Cochrane Database Syst Rev. 2016. PMID: 27030386 Free PMC article.
References
-
- Singh G., Keller A., Lucas K., Borders C., Stout D., King M., Parikh P., Stepp N., Ugiliweneza B., D’Amico J.M., et al. Safety and Feasibility of Cervical and Thoracic Transcutaneous Spinal Cord Stimulation to Improve Hand Motor Function in Children with Chronic Spinal Cord Injury. Neuromodulation. 2024;27:661–671. doi: 10.1016/j.neurom.2023.04.475. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
