

Disease Severity- and Hormonal Status-Dependent Alterations of EGF and MIF in the Serum of Endometriosis Patients
- PMID: 40724945
- PMCID: PMC12294931
- DOI: 10.3390/ijms26146695
Disease Severity- and Hormonal Status-Dependent Alterations of EGF and MIF in the Serum of Endometriosis Patients
Abstract
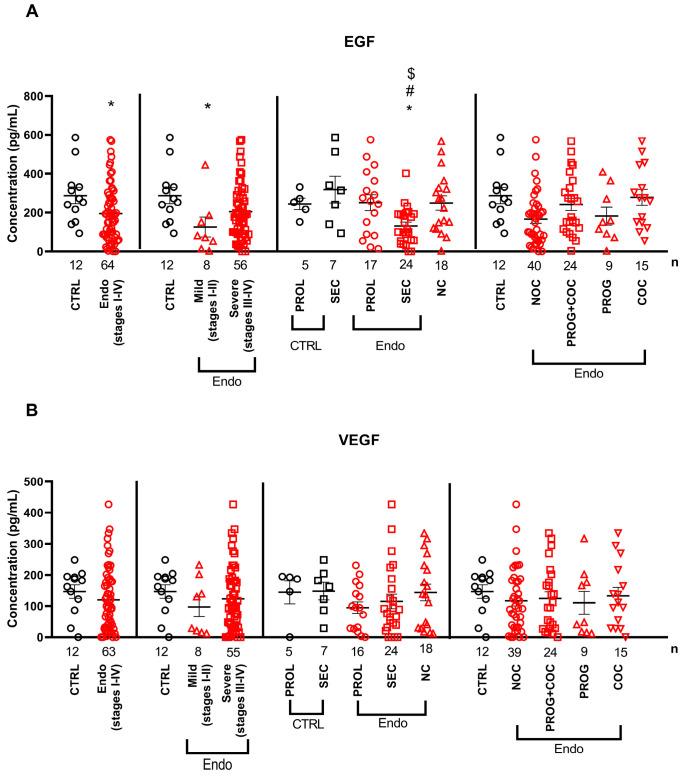
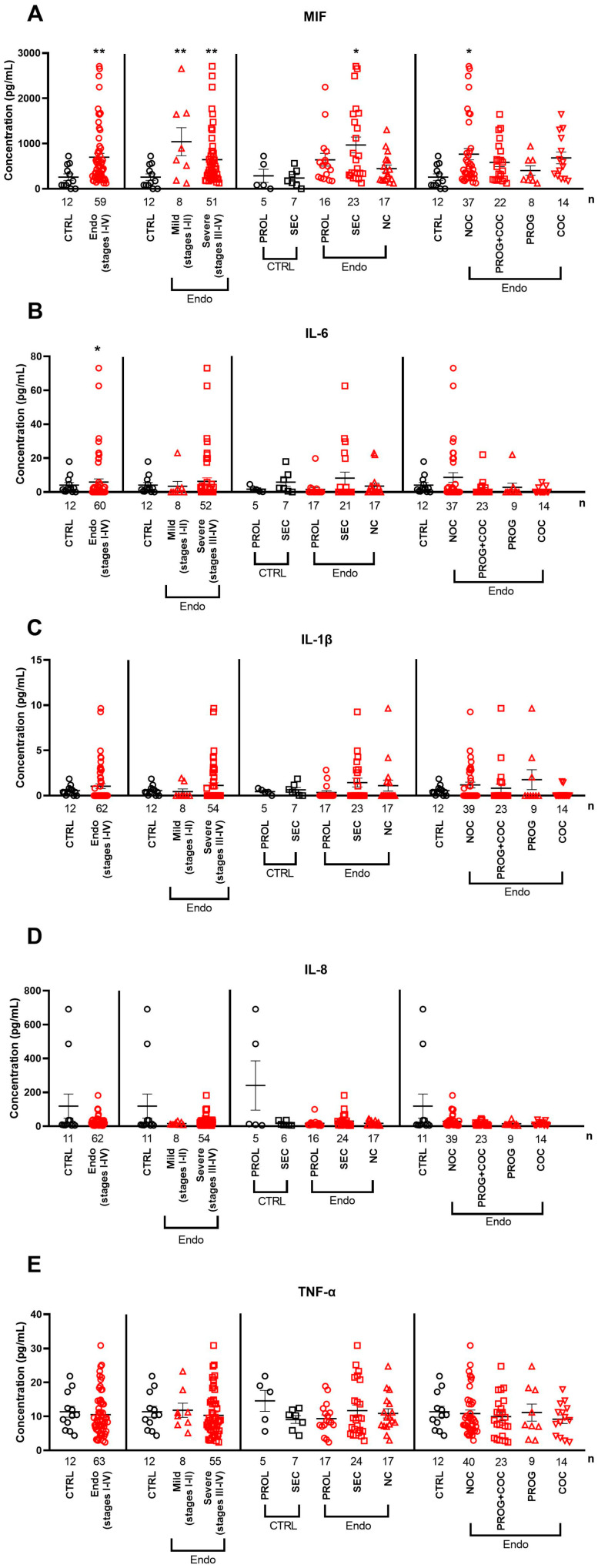
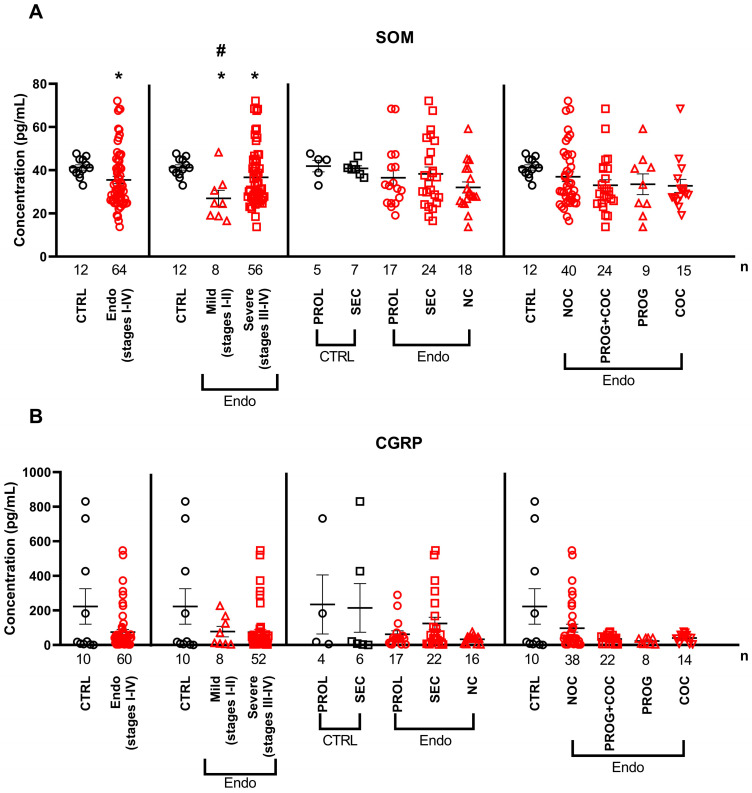
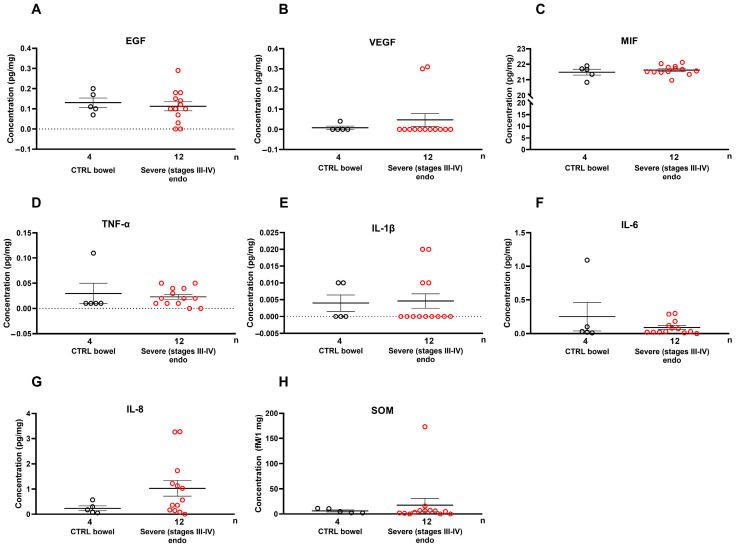
Endometriosis is the extrauterine engraftment of endometrium-like tissue, causing chronic pain. Complex sensory-vascular-immune interactions, including growth factors, cytokines, and neuropeptides, are implicated in its pathophysiology, but the mechanisms remain unknown. Here, epidermal growth factor (EGF), vascular endothelial growth factor, interleukins (IL-1β, IL-6, IL-8), macrophage migration inhibitory factor (MIF), calcitonin gene-related peptide, and somatostatin were measured in the serum of endometriosis patients with different disease severities, menstruation cycle- and pharmacotherapy-related hormonal status compared with controls. Mediator levels in deep-infiltrating rectosigmoid nodules were also compared with those in non-endometriotic colon tissues. Pain was assessed by the visual analogue scale. Serum EGF was significantly lower in mild endometriosis and in the secretory phase. MIF and IL-6 were higher in stage I-IV endometriosis, with MIF also higher in the secretory phase and in patients not receiving oral contraceptives. Somatostatin was lower in mild endometriosis than that in healthy individuals and the severe endometriosis group. No tissue-level differences were found. A strong positive correlation between serum EGF and somatostatin levels and dysmenorrhea and dysuria was detected in mild cases. It is concluded that certain serum alterations may be related to severity- and hormone status-dependent endometriosis mechanisms, but their diagnostic/prognostic value seems to be limited due to variability and lack of specificity.
Keywords: calcitonin gene-related peptide; endometriosis; immunoassay; interleukins; macrophage migration inhibitory factor; pain assessment; somatostatin; systemic inflammation; tumor necrosis factor alpha; visual analogue scale.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Zsuzsanna Helyes is the founder of PharmInVivo Ltd., Pécs, Hungary, but the company had no role in designing or funding this study; in data collection, analyses, or interpretation; in writing the manuscript; or in publishing the results.
Figures
References
-
- Simoens S., Dunselman G., Dirksen C., Hummelshoj L., Bokor A., Brandes I., Brodszky V., Canis M., Colombo G.L., Deleire T., et al. The burden of endometriosis: Costs and quality of life of women with endometriosis and treated in referral centres. Hum. Reprod. 2012;27:1292–1299. doi: 10.1093/humrep/des073. - DOI - PubMed
-
- Keckstein J., Saridogan E., Ulrich U.A., Sillem M., Oppelt P., Schweppe K.W., Krentel H., Janschek E., Exacoustos C., Malzoni M., et al. The #Enzian classification: A comprehensive non-invasive and surgical description system for endometriosis. Acta Obstet. Gynecol. Scand. 2021;100:1165–1175. - PubMed
MeSH terms
Substances
Grants and funding
- RRF-2.3.1-21-2022-00015/National Research, Development and Innovation Office
- Hungarian Research Network (HUN-REN)
- TKP2021-EGA-13/Ministry of Culture and Innovation of Hungary from the National Research, Development and Innovation Fund
- "Dr. Szolcsányi János" GYTK KA-2024-02
- OTKA- NKFIH K 138046/National Research, Development and Innovation Office
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
