

Iliac Stemmed Cups: A Review of History, Indications, and Clinical Outcomes in Revision Hip Arthroplasty and Primary Severe Dysplasia
- PMID: 40725648
- PMCID: PMC12295581
- DOI: 10.3390/jcm14144955
Iliac Stemmed Cups: A Review of History, Indications, and Clinical Outcomes in Revision Hip Arthroplasty and Primary Severe Dysplasia
Abstract
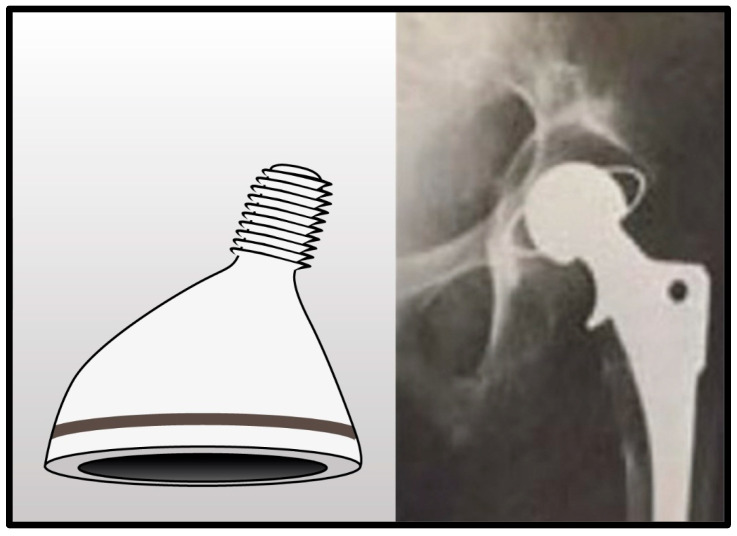
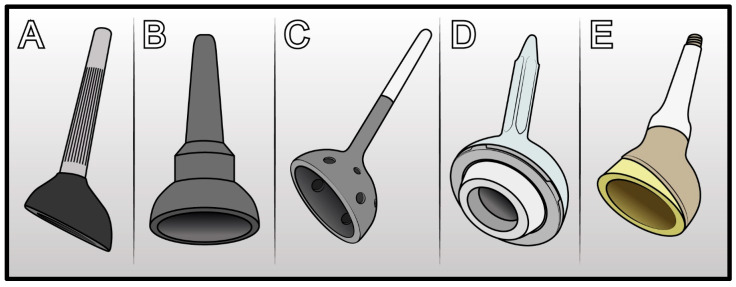
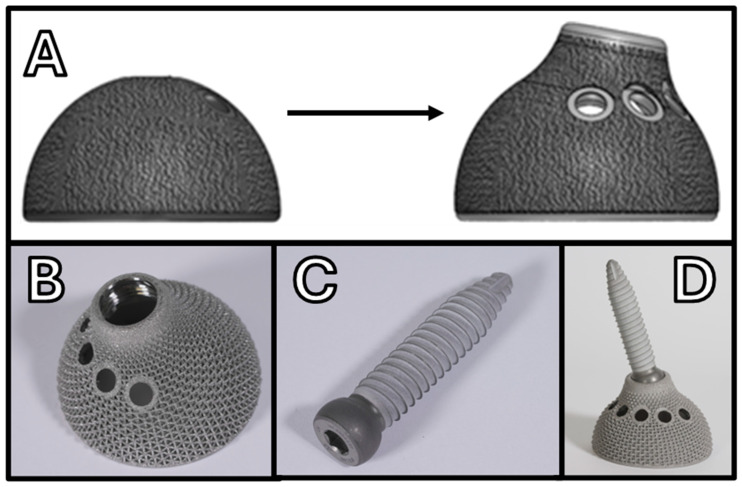
Background: The increasing incidence of revision total hip arthroplasties (rTHAs), particularly due to failure of the acetabular components and severe bone loss, necessitates reliable surgical solutions. Iliac stemmed cups (ISCs) have emerged as effective options for managing complex pelvic defects, including Paprosky type 3A and 3B acetabular defects, severe developmental dysplasia, and selected pelvic discontinuities. This review examines the historical evolution, clinical indications, and outcomes associated with ISCs. Methods: This narrative review analyzed the historical and recent literature concerning various ISC designs. We critically assessed clinical outcomes, complication rates, and implant survival from 13 key studies. Results: ISCs have progressed significantly from initial monobloc designs to contemporary modular configurations, substantially enhancing surgical versatility and biomechanical stability. Clinical outcomes varied with reported complications such as infection, dislocation, mechanical failure, and aseptic loosening ranging from 10% to over 30%. Newer modular implants like the Sansone cup have demonstrated improved outcomes, with complication rates below 10% and five-year survival rates exceeding 95%. Conclusions: ISCs are reliable and versatile implants, particularly suited to address significant pelvic bone deficiencies. Optimal surgical techniques and careful implant selection remain essential to minimize complications and achieve favorable long-term functional outcomes, making these implants valuable tools in complex hip arthroplasty.
Keywords: Iliac stemmed cup; acetabular bone loss; developmental hip dysplasia; pelvic reconstruction; revision THA; revision hip arthroplasty.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







Similar articles
-
What Are the Functional, Radiographic, and Survivorship Outcomes of a Modified Cup-cage Technique for Pelvic Discontinuity?Clin Orthop Relat Res. 2024 Dec 1;482(12):2149-2160. doi: 10.1097/CORR.0000000000003186. Epub 2024 Jul 9. Clin Orthop Relat Res. 2024. PMID: 38991223
-
Dual-mobility arthroplasty failure: a rationale review of causes and technical considerations for revision.Int Orthop. 2017 Mar;41(3):481-490. doi: 10.1007/s00264-016-3328-7. Epub 2016 Nov 21. Int Orthop. 2017. PMID: 27872981
-
Hip arthroplasty for acute femoral neck fracture: Hemiarthroplasty, dual mobility, or conventional total hip arthroplasty? A comparative analysis of 37,169 hip arthroplasties from the Swiss National Joint Registry.Orthop Traumatol Surg Res. 2025 Jul 9:104331. doi: 10.1016/j.otsr.2025.104331. Online ahead of print. Orthop Traumatol Surg Res. 2025. PMID: 40645446
-
Trabecular metal versus non-trabecular metal acetabular components for acetabular revision surgery: A systematic review and meta-analysis.Int J Surg. 2022 Apr;100:106597. doi: 10.1016/j.ijsu.2022.106597. Epub 2022 Mar 11. Int J Surg. 2022. PMID: 35288338
-
Is 18 F-fluoride PET/CT an Accurate Tool to Diagnose Loosening After Total Joint Arthroplasty?Clin Orthop Relat Res. 2025 Mar 1;483(3):415-428. doi: 10.1097/CORR.0000000000003228. Epub 2024 Sep 11. Clin Orthop Relat Res. 2025. PMID: 39293088
References
-
- R.I.P.O Register of Orthopedic Prosthetic Implantology, Emilia Romagna. [(accessed on 1 November 2024)]. Available online: https://ripo.cineca.it/authzssl/index.htm.
Publication types
LinkOut - more resources
Full Text Sources
