

Intramedullary nailing using K-wires for high-energy distal humeral metaphyseal-diaphyseal fractures accompanying radial nerve palsy in a 2-year-old toddler: A case report
- PMID: 40725908
- PMCID: PMC12303419
- DOI: 10.1097/MD.0000000000043322
Intramedullary nailing using K-wires for high-energy distal humeral metaphyseal-diaphyseal fractures accompanying radial nerve palsy in a 2-year-old toddler: A case report
Abstract
Rationale: Pediatric distal humeral diaphyseal fractures are rare and challenging to manage due to anatomical and biomechanical complexities. In addition, humeral shaft fractures in adults are often accompanied by radial nerve paralysis (RNP), but there are no studies on the incidence or treatment of pediatric humeral shaft fractures accompanied by RNP in toddlers. The authors present the outcomes of closed reduction and intramedullary nailing using Kirschner wires (K-wires) for high-energy distal humeral metaphyseal-diaphyseal open fractures accompanied by RNP in a toddler. This case report aims to highlight an effective surgical approach and its outcomes in a toddler, providing insights for clinicians facing similar scenarios.
Patient concerns: A 23-month-old boy was referred to our emergency room after several hospital visits. He complained of pain in his right arm and presented wrist drop due to a crushing injury by a conveyor belt. A 1 cm open wound was located at the lateral side of the elbow.
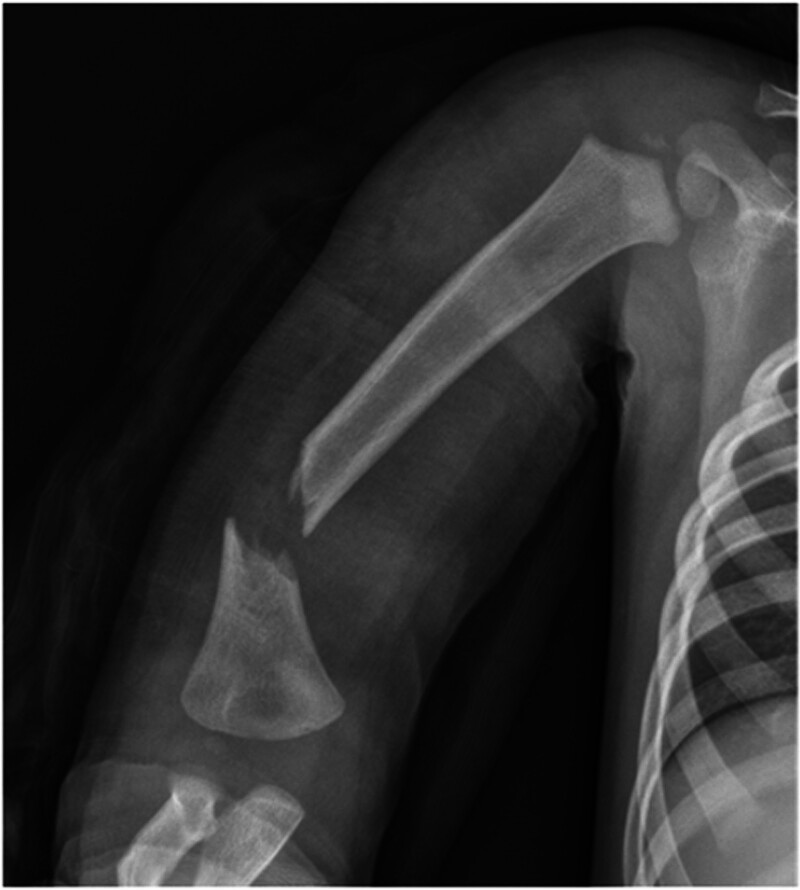
Diagnosis: The patient was diagnosed with an open displaced fracture in the distal third of the right humerus on radiographic examination and RNP was diagnosed on the basis of physical examination.
Interventions: The authors initially attempted open reduction and internal fixation of the fracture using a Steinmann pin after radial nerve exploration, which confirmed continuity of the normal radial nerve, but fixation failed. Reduction loss and displacement progressed with pin migration the day after surgery, and revision surgery was selected. Closed reduction and intramedullary nailing using K-wires were performed on day 2 after the primary surgery.
Outcomes: The patient recovered his ability to extend the wrist and metacarpophalangeal joint approximately 3 weeks after surgery. At the 1-month and 6-month follow-up, the fracture had healed, and radial nerve function had recovered completely.
Lessons: Intramedullary nailing using K-wires for metaphyseal-diaphyseal fractures of the humerus in toddlers is an effective operative treatment. Among them, high-energy open fractures accompanied by radial nerve palsy might require nerve exploration.
Keywords: distal humeral metaphyseal–diaphyseal fracture; high-energy injury; intramedullary nailing; pediatric open humeral fracture; radial nerve palsy; toddler.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures




Similar articles
-
Incidence and outcomes of radial nerve palsy in distal third diaphyseal humerus fractures after surgical fixation.Eur J Orthop Surg Traumatol. 2025 Jul 30;35(1):330. doi: 10.1007/s00590-025-04462-7. Eur J Orthop Surg Traumatol. 2025. PMID: 40736753
-
Dynamic compression plating versus locked intramedullary nailing for humeral shaft fractures in adults.Cochrane Database Syst Rev. 2011 Jun 15;(6):CD005959. doi: 10.1002/14651858.CD005959.pub2. Cochrane Database Syst Rev. 2011. PMID: 21678350
-
Interventions for treating supracondylar elbow fractures in children.Cochrane Database Syst Rev. 2022 Jun 9;6(6):CD013609. doi: 10.1002/14651858.CD013609.pub2. Cochrane Database Syst Rev. 2022. PMID: 35678077 Free PMC article.
-
Intramedullary nailing for tibial shaft fractures in adults.Cochrane Database Syst Rev. 2012 Jan 18;1(1):CD008241. doi: 10.1002/14651858.CD008241.pub2. Cochrane Database Syst Rev. 2012. PMID: 22258982 Free PMC article.
-
Interventions for treating femoral shaft fractures in children and adolescents.Cochrane Database Syst Rev. 2014 Jul 29;2014(7):CD009076. doi: 10.1002/14651858.CD009076.pub2. Cochrane Database Syst Rev. 2014. PMID: 25072888 Free PMC article.
References
-
- Rennie L, Court-Brown CM, Mok JY, Beattie TF. The epidemiology of fractures in children. Injury. 2007;38:913–22. - PubMed
-
- Caviglia H, Garrido CP, Palazzi FF, Meana NV. Pediatric fractures of the humerus. Clin Orthop Relat Res. 2005;432:49–56. - PubMed
-
- Fayssoux RS, Stankovits L, Domzalski ME, Guille JT. Fractures of the distal humeral metaphyseal-diaphyseal junction in children. J Pediatr Orthop. 2008;28:142–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
