

Olmesartan-Induced Gastropathy: An Important Cause to Think about in Refractory Peptic Ulcer Disease
- PMID: 40726554
- PMCID: PMC12296203
- DOI: 10.1159/000543202
Olmesartan-Induced Gastropathy: An Important Cause to Think about in Refractory Peptic Ulcer Disease
Abstract
Background: Angiotensin receptor blockers are a pharmacological class widely used as antihypertensive therapy. Recently, a relationship between these agents and gastrointestinal disease has been described, namely, enteropathy, gastropathy, and microscopic colitis. The mechanism is unknown, but it is thought that a cell-mediated immune reaction is involved and does not appear to be a class effect. Treatment consists of stopping the drug and rechallenge can confirm the diagnosis.
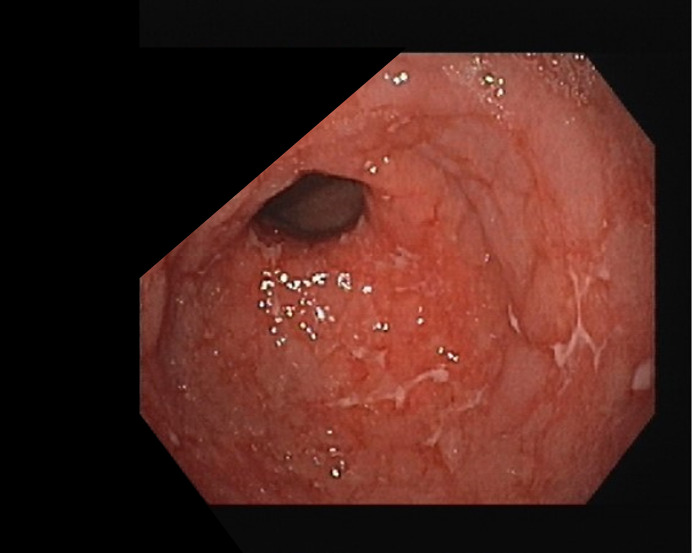
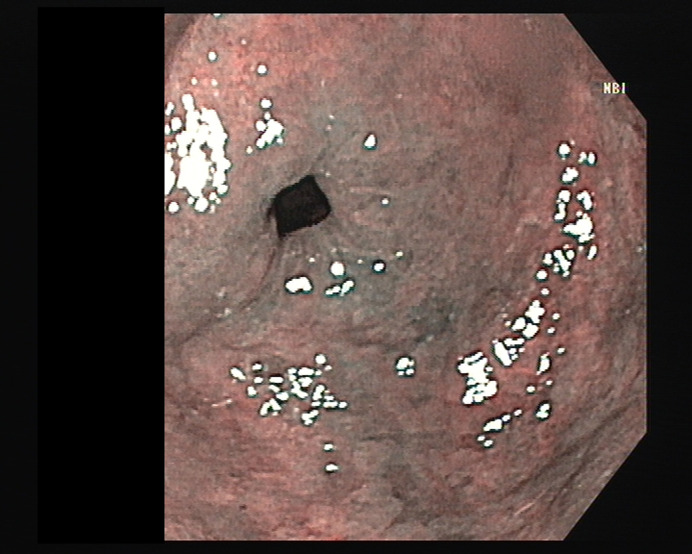
Case presentation: An 85-year-old man with a history of hypertension treated with olmesartan/hydrochlorothiazide for 12 years presented to the emergency department with months of epigastric pain, without vomiting, blood loss, diarrhea, or weight loss. A recent upper gastrointestinal endoscopy (UGE) showed congested mucosa, irregular erosions, and friability in the distal body, notch, and antrum. Histology revealed moderate chronic gastritis, severe inflammatory activity, abundant eosinophils, intestinal metaplasia with low-grade dysplasia, and marked atrophy, with no signs of malignancy or Helicobacter pylori (Hp). The patient had previously been treated by his family doctor with lansoprazole and sucralfate, without improvement, and was subsequently discharged on esomeprazole with a referral for a gastroenterology consultation. Three months later, a follow-up UGE showed persistent erosions despite good adherence to esomeprazole. Hp serology was positive, and the patient was started on bismuth-based quadruple therapy. A post-treatment urea breath test confirmed Hp eradication. Six months later, UGE still showed multiple ulcers in the distal body and antrum. Olmesartan was switched to lisinopril, and after another 6 months, a follow-up UGE showed no ulcers or erosions. Biopsies revealed reduced inflammation and no dysplasia, indicating histological improvement. Olmesartan-induced gastropathy was diagnosed.
Conclusions: This case report illustrates olmesartan-induced gastropathy, an important diagnosis to consider in cases of non-Hp gastritis and refractory peptic ulcer disease.
Introdução: Os antagonistas dos recetores da angiotensina são uma classe farmacológica amplamente utilizada como terapêutica anti-hipertensiva. Recentemente, foi descrita uma relação entre estes agentes e doenças gastrointestinais, nomeadamente enteropatia, gastropatia e colite microscópica. O mecanismo é desconhecido, mas acredita-se que envolva uma reação imune mediada por células e não parece ser um efeito de classe. O tratamento consiste na suspensão do fármaco, e a reexposição pode confirmar o diagnóstico.
Apresentação do caso: Um homem de 85 anos, com antecedentes de hipertensão arterial tratada com olmesartan/hidroclorotiazida há 12 anos, recorreu ao serviço de urgência por dor epigástrica persistente com vários meses de evolução, sem episódios de vómitos, perdas de sangue, diarreia ou perda de peso. Uma endoscopia digestiva alta (EDA) recente revelou mucosa congestiva, erosões irregulares e friabilidade no corpo distal, incisura e antro gástrico. A histologia mostrou uma gastrite crónica moderada, com elevada atividade inflamatória, eosinófilos abundantes, metaplasia intestinal com displasia de baixo grau e atrofia acentuada, sem sinais de malignidade ou de Hp. O doente já tinha previamente sido medicado pelo seu médico de família com lansoprazol e sucralfato, sem melhoria, e acabou por ter alta com esomeprazol e um pedido de consulta de gastrenterologia. Três meses depois, uma nova EDA revelou erosões persistentes, apesar da boa adesão ao esomeprazol. A serologia para Hp foi positiva, e foi iniciada erradicação com terapêutica quádrupla com bismuto. Um teste de respiração de ureia pós-tratamento confirmou a erradicação do Hp. Seis meses depois, a EDA ainda mostrou múltiplas úlceras no corpo distal e no antro gástrico. O olmesartan foi substituído pelo lisinopril, e após mais seis meses, uma nova EDA não demonstrou úlceras nem erosões. As biópsias mostraram uma redução da inflamação e ausência de displasia, indicando uma melhoria histológica. Assumiu-se o diagnóstico de gastropatia induzida por olmesartan.
Conclusões: Este relato de caso ilustra a gastropatia induzida por olmesartan, um diagnóstico importante a considerar em casos de gastrite não associada a Hp e doença ulcerosa péptica refratária.
Keywords: Angiotensin receptor blockers; Drug-induced gastropathy; Refractory peptic ulcer disease.
© 2024 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Costetti M, Schiepatti A, Fraticelli S, Costa S, Maimaris S, Lenti MV, et al. Clinical and gastro-duodenal histopathological features of enteropathy due to angiotensin II receptor blockers. Dig Liver Dis. 2021;53(10):1262–7. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
