

Usefulness of A Portal Vein Stent for Sinistral Portal Hypertension: A Case Report
- PMID: 40726829
- PMCID: PMC12303666
- DOI: 10.70352/scrj.cr.25-0206
Usefulness of A Portal Vein Stent for Sinistral Portal Hypertension: A Case Report
Abstract
Introduction: Portal vein (PV) and splenic vein (SV) stenosis are known complications of pancreatoduodenectomy (PD) and often lead to portal hypertension. PV stenosis extending to the SV confluence can result in sinistral portal hypertension (SPH), characterized by gastrointestinal varices and splenomegaly in the presence of normal liver function. There is no standardized treatment strategy for SPH following PD.
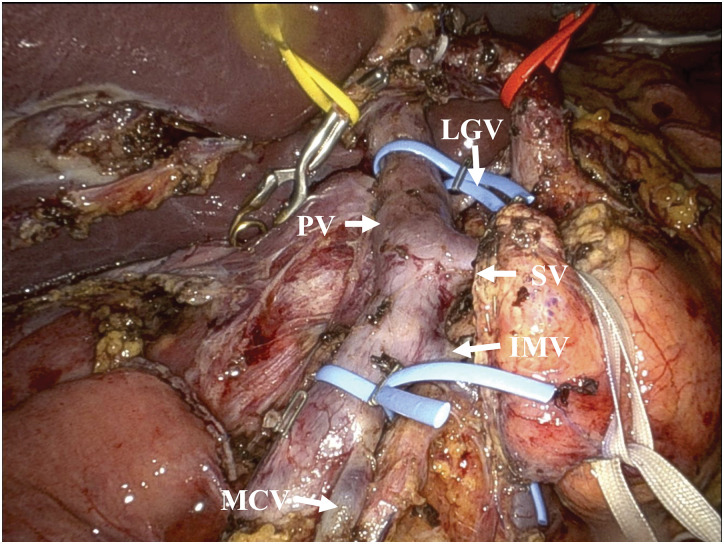
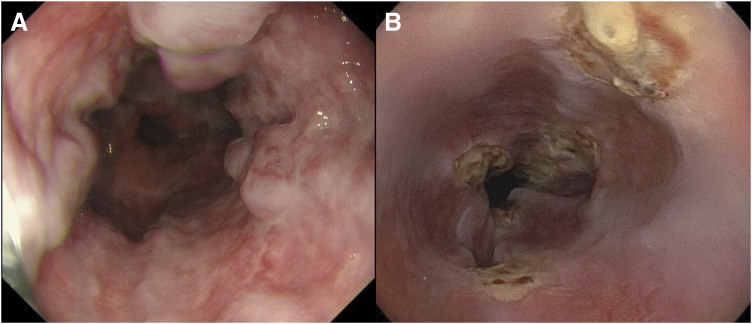
Case presentation: A 42-year-old female underwent robot-assisted PD for a pancreatic neuroendocrine tumor without immediate PV complications. Postoperatively, the patient experienced fluid retention; however, this did not pose a problem, and no therapeutic intervention was necessary. Two months later, imaging revealed PV stenosis and SV obstruction. Eleven months after surgery, the patient presented with melena, and imaging confirmed the presence of gastroesophageal varices with severe PV stenosis and complete SV obstruction. Endoscopic variceal ligation was performed, and the hemodynamic status of the portal system was assessed using computed tomography during arterial portography (CTAP). CTAP showed communication between the superior mesenteric vein and the SV via the middle colic vein. Therefore, we decided to perform PV stenting. The stent was successfully placed, resulting in a significant improvement in the esophageal varices. The patient was discharged on postoperative day 4, receiving anticoagulant therapy, with no further complications.
Conclusions: This case demonstrates the efficacy of PV stenting after careful hemodynamic assessment in a patient who developed SPH due to PV stenosis and SV obstruction following PD.
Keywords: pancreatoduodenectomy; portal vein stenosis; portal vein stent; sinistral portal hypertension; splenic vein stenosis.
© 2025 The Author(s). Published by Japan Surgical Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
Case report and systematic literature review of a novel etiology of sinistral portal hypertension presenting with UGI bleeding: Left gastric artery pseudoaneurysm compressing the splenic vein treated by embolization of the pseudoaneurysm.Medicine (Baltimore). 2017 Mar;96(13):e6413. doi: 10.1097/MD.0000000000006413. Medicine (Baltimore). 2017. PMID: 28353569 Free PMC article.
-
Endoscopic injection of cyanoacrylate glue versus other endoscopic procedures for acute bleeding gastric varices in people with portal hypertension.Cochrane Database Syst Rev. 2015 May 12;2015(5):CD010180. doi: 10.1002/14651858.CD010180.pub2. Cochrane Database Syst Rev. 2015. PMID: 25966446 Free PMC article.
-
Platelet count, spleen length, and platelet count-to-spleen length ratio for the diagnosis of oesophageal varices in people with chronic liver disease or portal vein thrombosis.Cochrane Database Syst Rev. 2017 Apr 26;4(4):CD008759. doi: 10.1002/14651858.CD008759.pub2. Cochrane Database Syst Rev. 2017. PMID: 28444987 Free PMC article.
-
Implications of portal vein/superior mesenteric vein involvement in pancreatic cancer: A comprehensive correlation from preoperative radiological assessment to resection, pathology, and long-term outcomes. A retrospective cohort study.Int J Surg. 2025 Apr 1;111(4):2962-2972. doi: 10.1097/JS9.0000000000002307. Int J Surg. 2025. PMID: 39998570 Free PMC article.
-
Hepatic infarction occurred after 125I particle stent treatment for hepatocellular carcinoma with portal vein tumor thrombus: A case report.J Cancer Res Clin Oncol. 2024 Jun 17;150(6):308. doi: 10.1007/s00432-024-05826-y. J Cancer Res Clin Oncol. 2024. PMID: 38884802 Free PMC article.
References
-
- Kang MJ, Jang JY, Chang YR, et al. Portal vein patency after pancreatoduodenectomy for periampullary cancer. Br J Surg 2015; 102: 77–84. - PubMed
-
- Fujii T, Nakao A, Yamada S, et al. Vein resections >3 cm during pancreatectomy are associated with poor 1-year patency rates. Surgery 2015; 157: 708–15. - PubMed
-
- Kim KR, Ko GY, Sung KB, et al. Percutaneous transhepatic stent placement in the management of portal venous stenosis after curative surgery for pancreatic and biliary neoplasms. AJR Am J Roentgenol 2011; 196: W446–50. - PubMed
-
- Novellas S, Denys A, Bize P, et al. Palliative portal vein stent placement in malignant and symptomatic extrinsic portal vein stenosis or occlusion. Cardiovasc Intervent Radiol 2009; 32: 462–70. - PubMed
-
- Evans GR, Yellin AE, Weaver FA, et al. Sinistral (left-sided) portal hypertension. Am Surg 1990; 56: 758–63. - PubMed