

Stereotactic Radiosurgery for a Patient With 94 Brain Metastases in the Setting of Prior Whole Brain Radiation
- PMID: 40726868
- PMCID: PMC12303361
- DOI: 10.7759/cureus.86925
Stereotactic Radiosurgery for a Patient With 94 Brain Metastases in the Setting of Prior Whole Brain Radiation
Abstract
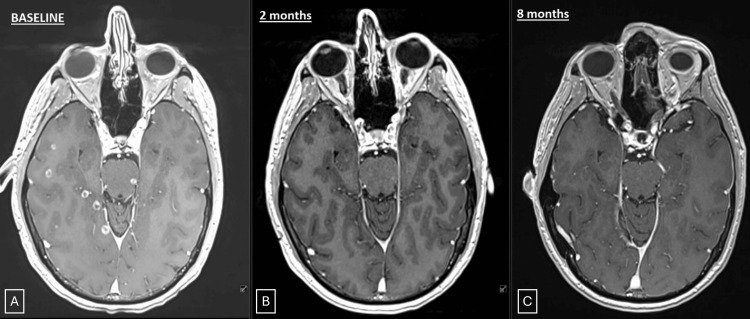
The current standard of care treatment for patients with ≥15 brain metastases (BM) is whole brain radiation therapy (WBRT), despite poor neurocognitive outcomes. Here, we present our experience treating a young patient with 94 intact brain metastases with SRS in the setting of prior WBRT. A 37-year-old male with metastatic lung adenocarcinoma (PD-L1 5%, EGFR exon 19 deletion) initially presented with a seizure and numerous intracranial metastases and previously completed a course of WBRT to a total dose of 3000 cGy in 10 fractions at an outside hospital. He subsequently started first-line oral osimertinib therapy, with baseline PET/CT showing multiple sites of disease. After 18 months from initial diagnosis and WBRT, the patient presented with 94 new brain metastases while on maintenance osimertinib. He had a Karnofsky performance score of 90, no neurological deficits, and only occasional headaches. His baseline cognitive objective Patient-Reported Outcome Measurement Information System (PROMIS) score was 29/40. Given his age, failure of EGFR-targeted therapy, and prior WBRT, he was planned for single-isocenter multiple target (SIMT) fractionated SRS to all lesions to a total dose of 2400 cGy in three fractions to 91 lesions and 1800 cGy to three brainstem metastases. He was simulated with a Qfix© Encompass mask (Qfix, Avondale, PA, USA) and treated on a Varian Edge linear accelerator utilizing HyperArc (Varian, Palo Alto, CA, USA), a 6DOF robotic couch with daily CBCT, and a Varian Optical Surface Monitoring System. A planning target volume (PTV) was created using a 2 mm margin around the GTV, with a smaller margin of 1 mm for brainstem metastases. The total GTV was 8.6 cc and PTV was 40.1 cc. He tolerated SRS well with no acute side effects. Due to progressive systemic disease, he transitioned to atezolizumab, paclitaxel, carboplatin, and bevacizumab combination therapy. Follow-up MRI imaging at two and five months was consistent with post-treatment changes, with no increase in the volume or number of brain metastases. His serial PROMIS scores were 29, 29, and 26 at three, six, and nine months of follow-up, respectively. At the last follow-up, 11 months after SRS, he remained free of headaches or new neurological symptoms. Due to the systemic progression of the disease, he transitioned to comfort care 30 months after BM diagnosis and 11 months after SRS. This case illustrates one of the largest numbers of metastases treated in a single course of SRS, and this treatment was well tolerated, with no significant cognitive decline, resulting in a comparable survival outcome to contemporary studies evaluating WBRT in this population.
Keywords: brain metastases with nsclc; egfr mutant lung adenocarcinoma; linac-based radiosurgery; osimertinib; radiation therapy; whole brain rt.
Copyright © 2025, Upadhyay et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

Similar articles
-
Single and multitarget stereotactic radiosurgery (SRS) with single isocenter in the treatment of multiple brain metastases (BM): institutional experience.Clin Transl Oncol. 2025 Jul;27(7):3183-3197. doi: 10.1007/s12094-024-03844-3. Epub 2025 Jan 15. Clin Transl Oncol. 2025. PMID: 39814975
-
Whole brain radiotherapy for the treatment of newly diagnosed multiple brain metastases.Cochrane Database Syst Rev. 2012 Apr 18;2012(4):CD003869. doi: 10.1002/14651858.CD003869.pub3. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2018 Jan 25;1:CD003869. doi: 10.1002/14651858.CD003869.pub4. PMID: 22513917 Free PMC article. Updated.
-
Whole brain radiation therapy (WBRT) alone versus WBRT and radiosurgery for the treatment of brain metastases.Cochrane Database Syst Rev. 2017 Sep 25;9(9):CD006121. doi: 10.1002/14651858.CD006121.pub4. Cochrane Database Syst Rev. 2017. PMID: 28945270 Free PMC article.
-
Whole brain radiation therapy (WBRT) alone versus WBRT and radiosurgery for the treatment of brain metastases.Cochrane Database Syst Rev. 2012 Sep 12;2012(9):CD006121. doi: 10.1002/14651858.CD006121.pub3. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2017 Sep 25;9:CD006121. doi: 10.1002/14651858.CD006121.pub4. PMID: 22972090 Free PMC article. Updated.
-
Radiotherapeutic management of brain metastases: a systematic review and meta-analysis.Cancer Treat Rev. 2005 Jun;31(4):256-73. doi: 10.1016/j.ctrv.2005.04.007. Cancer Treat Rev. 2005. PMID: 15951117
References
-
- Emerging systemic treatment perspectives on brain metastases: moving toward a better outlook for patients. Alvarez-Breckenridge C, Remon J, Piña Y, Nieblas-Bedolla E, Forsyth P, Hendriks L, Brastianos PK. Am Soc Clin Oncol Educ Book. 2022;42:1–19. - PubMed
-
- Association of long-term outcomes with stereotactic radiosurgery vs whole-brain radiotherapy for resected brain metastasis: a secondary analysis of the N107C/CEC.3 (Alliance for Clinical Trials in Oncology/Canadian Cancer Trials Group) randomized clinical trial. Palmer JD, Klamer BG, Ballman KV, et al. JAMA Oncol. 2022;8:1809–1815. - PMC - PubMed
-
- Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial. Chang E, Wefel J, Hess K, et al. Lancet Oncol. 2009;10:1037–1044. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous