

Dynamic versus fixed cerebral perfusion pressure targets in paediatric traumatic brain injury: a STARSHIP analysis
- PMID: 40727013
- PMCID: PMC12303001
- DOI: 10.1016/j.eclinm.2025.103370
Dynamic versus fixed cerebral perfusion pressure targets in paediatric traumatic brain injury: a STARSHIP analysis
Abstract
Background: Cerebral perfusion pressure (CPP) represents a key target for intensive care management of paediatric traumatic brain injury (TBI) patients. Current guidelines recommend a CPP target within the range of 40-50 mmHg but emphasise that these may depend on patient age and the state of cerebrovascular autoregulation. In this analysis, we aimed to compare the fixed targets proposed by the Brain Trauma Foundation to autoregulation-based targets CPPopt (optimal CPP) and LLA (Lower Limit of Autoregulation).
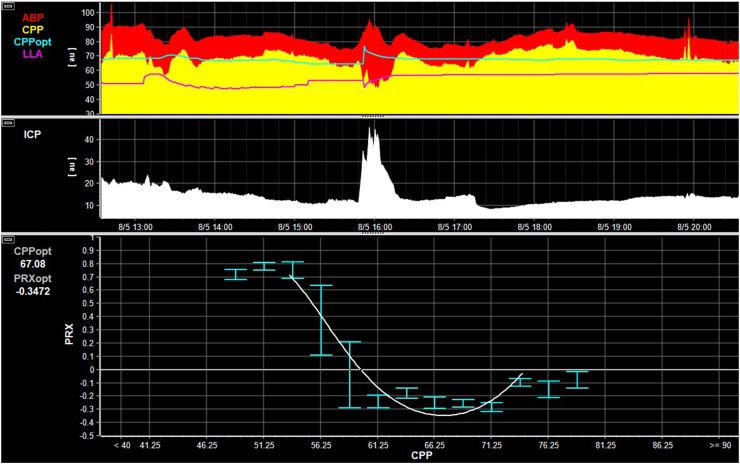
Methods: Data were acquired from the STARSHIP study (a prospective, multicentre, observational, research study which enrolled 135 children (median age 96 months (interquartile range 26-152 months)) with TBI between July 2018 and March 2023 across 10 paediatric intensive care units in the UK). In this secondary analysis the dose or percentage time spent below a fixed CPP target of 50 mmHg or CPPopt or LLA (assessed continuously on a minute-by-minute basis and derived by fitting a curve to the relationship between CPP and pressure reactivity index values, as previously described) was compared by outcome using univariable and multivariable methods. ClinicalTrials.gov registration-NCT0688462.
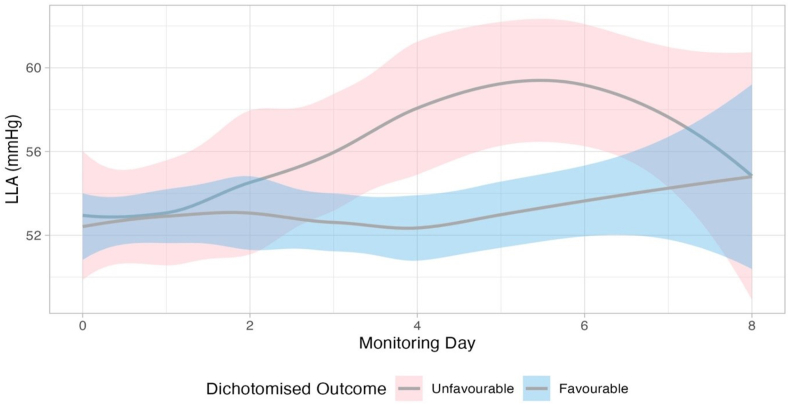
Findings: When assessed within ordinal analyses (to account for differences in baseline severity), both hourly dose and percentage time spent below LLA (odds ratio 1.01 [95% CI 1.00-1.02], p = 0.017 and 1.05 [95% CI 1.01-1.08], p = 0.008 respectively) were independently associated with worse outcomes. LLA displayed a dynamic time-trend increasing over time in patients with unfavourable outcome (n = 44, p = 0.003). Overall, LLA exceeded 50 mmHg for more than 45% of the monitoring period across all patients, and for over 35% of the time in the youngest cohort (0-2 years).
Interpretation: Dynamic autoregulation monitoring based on LLA was associated with outcomes in paediatric TBI with higher LLA values observed in individuals experiencing unfavourable outcomes. Our findings indicate that the current fixed CPP threshold of 40-50 mmHg may be too low-highlighting the need for further investigation into autoregulation-guided CPP targets. Whether personalised management based on autoregulatory-informed thresholds offers advantages over guideline-based targets remains to be determined and should be investigated in future prospective interventional studies.
Funding: Action Medical Research for Childrens' Charity and Addenbrookes Charitable Trust (UK Grant number-GN2609).
Keywords: Cerebral perfusion pressure; Cerebrovascular autoregulation; Intensive care management; Multimodality neuromonitoring; Paediatric traumatic brain injury.
© 2025 The Author(s).
Conflict of interest statement
The STARSHIP study was funded by Action Medical Research for Children's Charity and Addenbrookes Charitable Trust, UK (Grant number–GN2609). Cambridge University Hospitals is the study sponsor (Reference: A094693, contact person: Michelle Ellerbeck–michelle.ellerbeck@nhs.net). The funders or the sponsor did not have any role in the collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication, the right to veto publication or control the decision regarding which journal the manuscript was submitted. Stefan Yu Bögli is supported by the Swiss National Science Foundation (SNSF grant number: 225270). Claudia Ann Smith is supported by the Patrick & Margaret Flanagan Skye Cambridge Trust Scholarship. Erta Beqiri was supported by the Medical Research Council (grant number MR N013433-1) and by the Gates Cambridge Scholarship. Peter J Hutchinson is supported by the National Institute for Health Research (NIHR): research professorship, Biomedical Research Centre and Global Neurotrauma Research group and the Royal College of Surgeons of England. This research was supported by the NIHR Cambridge Biomedical Research Centre (NIHR203312∗). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. ICM+ is a software licenced by Cambridge Enterprise Ltd. Marek Czosnyka and Peter Smielewski have a financial interest in a part of licencing fee; the licencing fee was waived for this study.
Figures



References
-
- Kochanek P.M., Tasker R.C., Carney N., et al. Guidelines for the management of pediatric severe traumatic brain injury, third edition: update of the brain trauma foundation guidelines, executive summary. Neurosurgery. 2019;84(6):1169–1178. - PubMed
-
- Czosnyka M., Smielewski P., Kirkpatrick P., Menon D.K., Pickard J.D. Monitoring of cerebral autoregulation in head-injured patients. Stroke. 1996;27(10):1829–1834. - PubMed
-
- Czosnyka M., Smielewski P., Kirkpatrick P., Laing R.J., Menon D., Pickard J.D. Continuous assessment of the cerebral vasomotor reactivity in head injury. Neurosurgery. 1997;41(1):11–17. - PubMed
-
- Steiner L.A., Czosnyka M., Piechnik S.K., et al. Continuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury. Crit Care Med. 2002;30(4):733–738. - PubMed
LinkOut - more resources
Full Text Sources
