

Exploring personalized neoadjuvant therapy selection strategies in breast cancer: an explainable multi-modal response model
- PMID: 40727014
- PMCID: PMC12303063
- DOI: 10.1016/j.eclinm.2025.103356
Exploring personalized neoadjuvant therapy selection strategies in breast cancer: an explainable multi-modal response model
Abstract
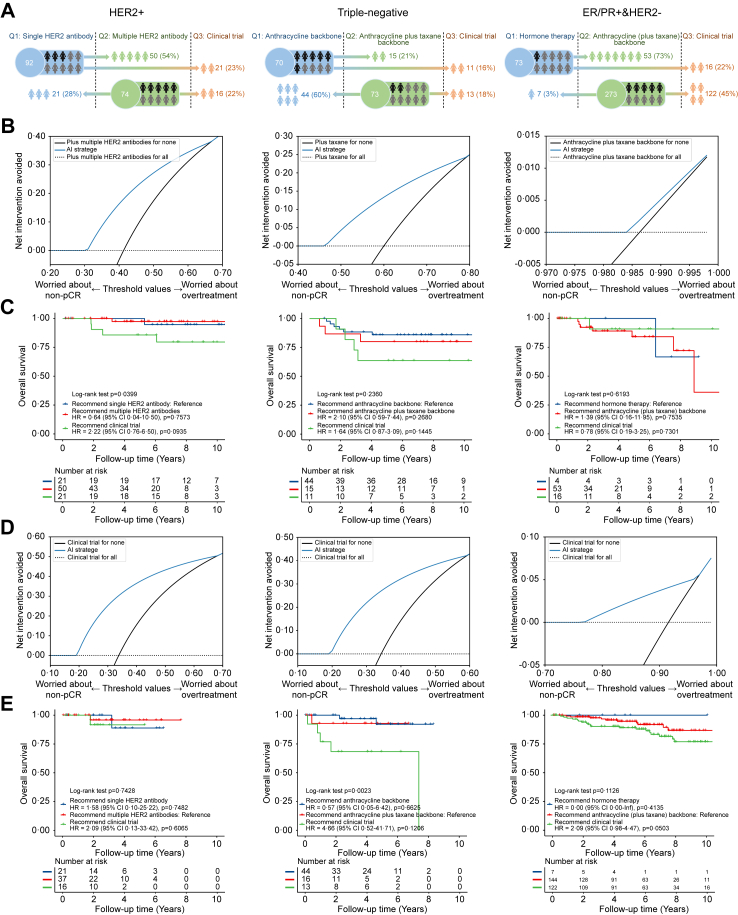
Background: Neoadjuvant therapy (NAT) regimens for breast cancer are generally determined according to cancer stage and molecular subtypes without fully considering the inter-patient variability, which may lead to inefficiency or overtreatment. Artificial intelligence (AI) may support personalized regimen recommendations by learning the synergistic relationship between pre-NAT individual-patient data, regimens, and corresponding short- or long-term therapy responses.
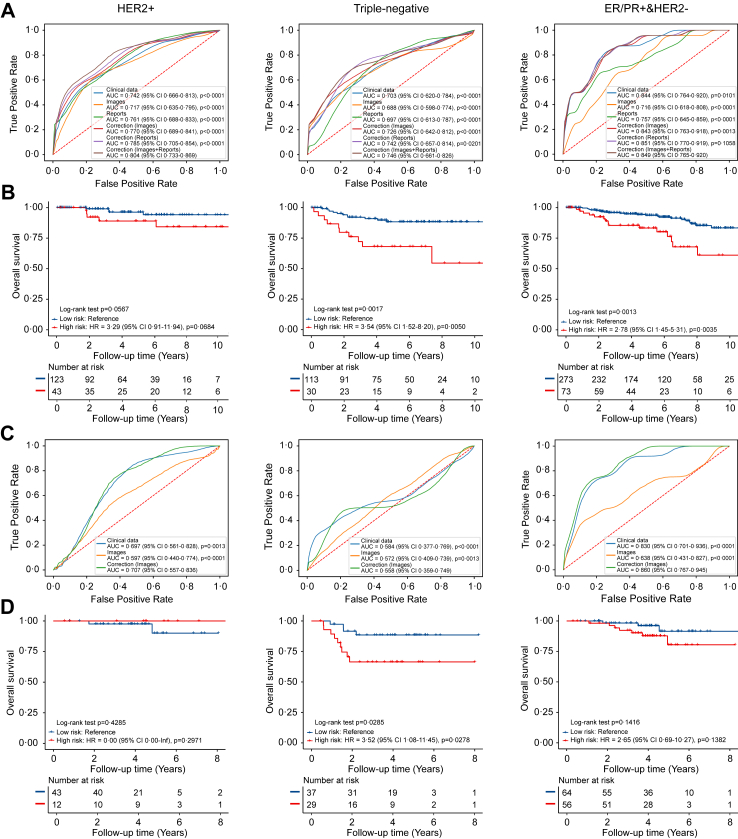
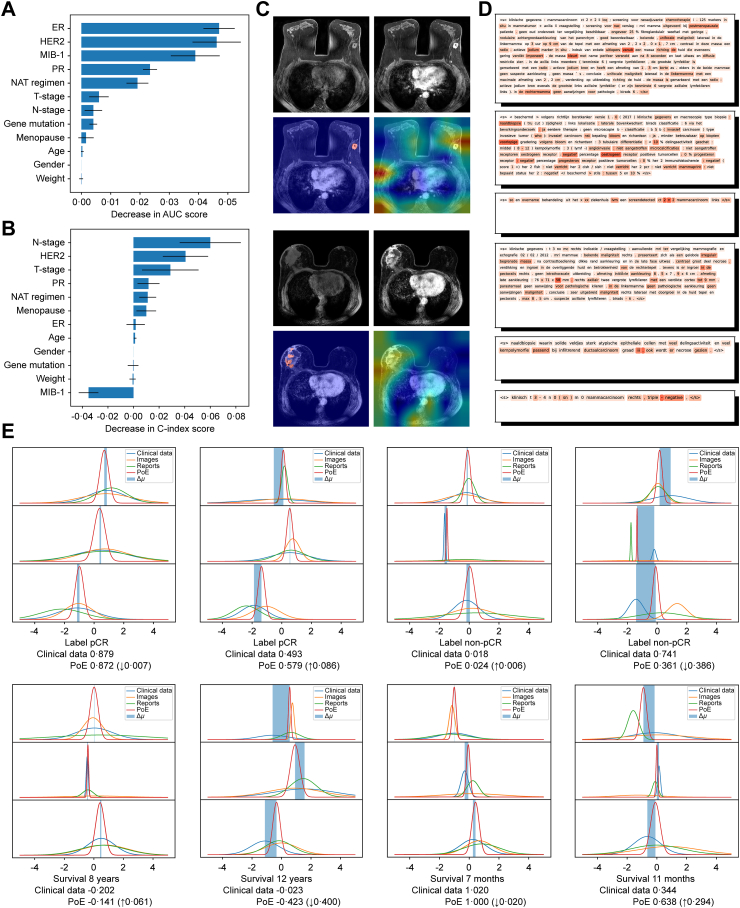
Methods: In this retrospective study, we collected data from breast cancer patients treated with NAT between 2000 and 2020 from the Netherlands and the USA. Median follow-up times ranged from 3·7 to 4·9 years across molecular subtypes and cohorts. We developed and externally validated a multi-modal model integrating pre-NAT clinical data, dynamic contrast enhanced (DCE)-MRI images, and medical reports to predict pathological complete response (pCR) and likelihood of survival after NAT. We subsequently evaluated potential benefits for patients receiving a personalized regimen recommended based on these predictions.
Findings: We trained our model on 655 patients and validated it on internal (655 patients) and external (241 patients) cohorts. Given the factual regimens, the model can correctly predict the corresponding therapy response, with areas under the receiver operating characteristic curves (AUC) of 0·80 (95% CI 0·73-0·87), 0·75 (0·66-0·83), and 0·85 (0·77-0·92) for pCR prediction of human epidermal growth factor receptor 2 (HER2)+, triple-negative, and estrogen receptor/progesterone receptor (ER/PR)+&HER2- patients in the internal validation cohort, respectively. Performance in the external validation cohort was 0·707 (0·557-0·836), 0·558 (0·359-0·749), and 0·860 (0·767-0·945) for the corresponding molecular subtypes, respectively. In the internal validation cohort, survival prediction identified high-risk patients across different molecular subtypes, as demonstrated by a hazard ratio (HR) of 3·29 (0·91-11·94) (HER2+), 3·54 (1·52-8·20) (triple-negative), and 2·78 (1·45-5·31) (ER/PR+&HER2-), albeit results were not significant for HER2+ cancers.
Interpretation: Our findings indicate that the prognostic scores generated by the response model could identify patient subgroups with relatively poor outcomes under their actual treatments. These preliminary findings may inform future efforts toward personalized NAT regimen selection beyond traditional criteria such as cancer stage and subtype, but should be interpreted cautiously and validated in prospective studies with longer follow-up because these tumors can relapse at a later stage.
Funding: None.
Keywords: Breast cancer; Explainable artificial intelligence; Multi-modal learning; Neoadjuvant therapy; Precise medicine.
© 2025 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Gradishar W.J., Moran M.S., Abraham J., et al. Breast cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2022;20:691–722. - PubMed
-
- Dubsky P., Pinker K., Cardoso F., et al. Breast conservation and axillary management after primary systemic therapy in patients with early-stage breast cancer: the Lucerne toolbox. Lancet Oncol. 2021;22:e18–e28. - PubMed
-
- Cortazar P., Zhang L., Untch M., et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384:164–172. - PubMed
-
- Broglio K.R., Quintana M., Foster M., et al. Association of pathologic complete response to neoadjuvant therapy in HER2-positive breast cancer with long-term outcomes: a meta-analysis. JAMA Oncol. 2016;2:751–760. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
