

Beyond direct visualization: a comparative analysis of computed tomography dacryocystographic features in dacryolithiasis, lacrimal sac cysts, and primary acquired nasolacrimal duct obstruction
- PMID: 40727344
- PMCID: PMC12290749
- DOI: 10.21037/qims-2024-2971
Beyond direct visualization: a comparative analysis of computed tomography dacryocystographic features in dacryolithiasis, lacrimal sac cysts, and primary acquired nasolacrimal duct obstruction
Abstract
Background: Dacryoliths occur in approximately 5.8-18% of patients undergoing dacryocystorhinostomy (DCR), but conventional diagnostic methods often fail to distinguish them from other causes of nasolacrimal duct obstruction (NLDO). This study aimed to analyze the characteristic features of dacryoliths on computed tomography dacryocystography (CT-DCG) and to establish imaging criteria for their differential diagnosis from lacrimal sac cysts and primary acquired nasolacrimal duct obstruction (PANDO).
Methods: In this retrospective case-control study, CT-DCG images from 54 patients (18 with surgically confirmed dacryoliths, 18 with lacrimal sac cysts, and 18 with PANDO) were analyzed. The assessment included lacrimal sac dimensions, contrast distribution patterns, and characteristic imaging features. For each case, the extent of contrast filling, surface irregularities, and presence of calcification were evaluated. Intraoperative findings and histopathological results were documented for dacryolith cases.
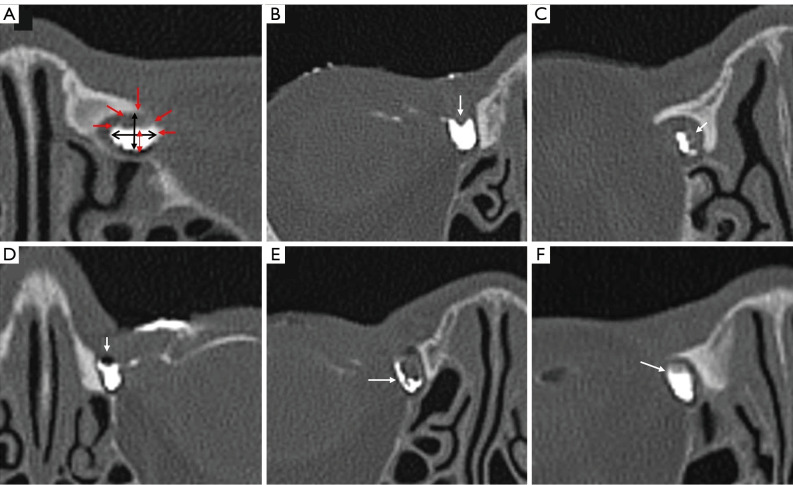
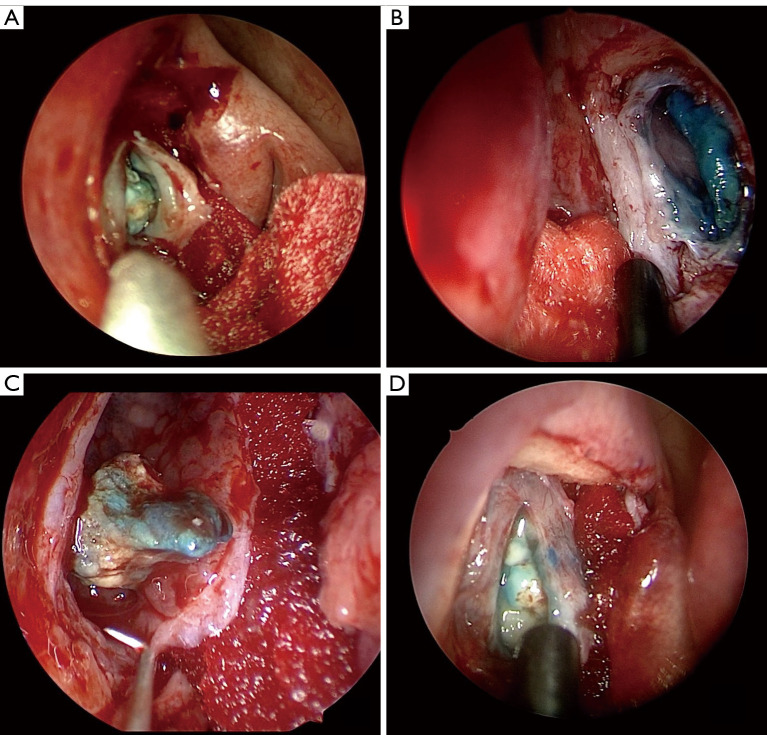
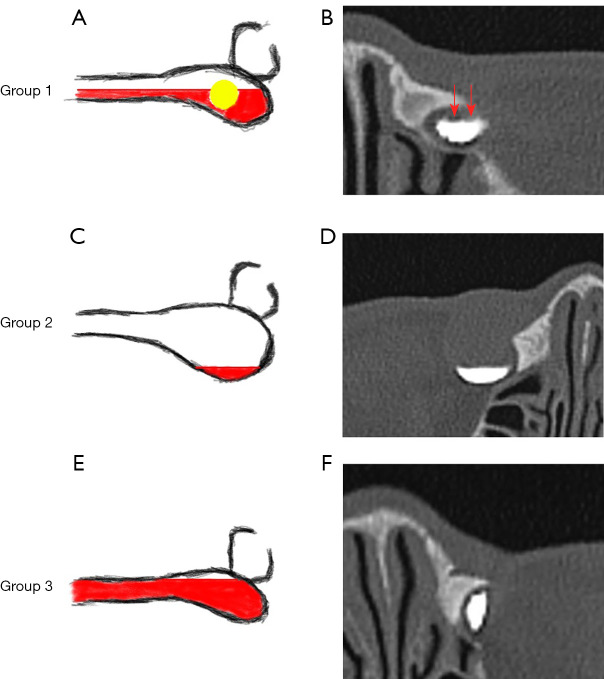
Results: Analysis of contrast distribution patterns on CT-DCG revealed significant differences between groups (P<0.01), with dacryolith cases showing characteristic moderate contrast filling (63.30%±20.43%), significantly different from the minimal filling in lacrimal sac cysts (29.44%±11.77%) and near-complete filling in PANDO cases (80.14%±15.46%). Dacryoliths demonstrated characteristic imaging features including surface filling defects (82.4%), peripheral calcification (64.7%), and density interface lines (23.5%). Lacrimal sac dimensions showed significant differences in both transverse and anteroposterior (AP) diameters (P<0.01), primarily due to enlargement in the lacrimal sac cyst group, while dacryolith and PANDO groups showed comparable measurements. Intraoperatively, combined sac-duct involvement was most common (44.4%), and histopathological examination revealed periodic acid Schiff-positive staining in 38.89% of dacryolith cases.
Conclusions: CT-DCG revealed characteristic contrast distribution patterns in dacryolithiasis, with moderate contrast filling that differed significantly from the filling of both lacrimal sac cysts and PANDO. When combined with surface filling defects, peripheral calcification, or density interface lines, these imaging features may serve as valuable diagnostic indicators for preoperative detection of dacryoliths.
Keywords: Dacryolith; computed tomography dacryocystography (CT-DCG); lacrimal sac cyst; mucopeptide concretions; primary acquired nasolacrimal duct obstruction (PANDO).
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-2024-2971/coif). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources