

Retrospective assessment of the frequency of cancer in the population of kidney transplant recipients - the experience of two transplant centers
- PMID: 40727470
- PMCID: PMC12301213
- DOI: 10.3389/fonc.2025.1497691
Retrospective assessment of the frequency of cancer in the population of kidney transplant recipients - the experience of two transplant centers
Abstract
Introduction: Cancer is one of the main causes of death among kidney recipients. The risk of cancer in kidney transplant recipients (KTRs) is 2-3 times higher as compared to the general population.
Aim: Retrospective assessment of the occurrence of cancer in the population of KTRs - based on data from two transplant centers.
Material: The study included a total of 246 KTRs, transplanted between 1980 and 2021, who were diagnosed with malignancy (the study did not include patients whose only cancer was non-melanoma skin cancer; NMSC).
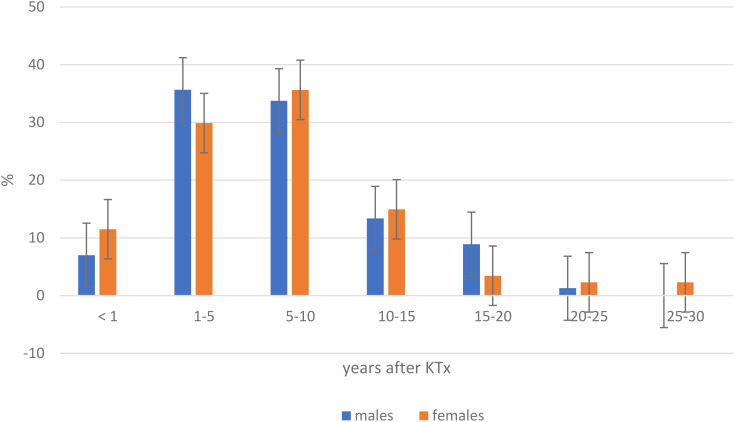
Results: 261 malignant tumors were diagnosed in 246 KTRs, 3 tumor was a recurrence, and the rest occurred de novo. The most common cancers in women were breast cancers (17.8%), colon cancers (14.5%), lung cancers and post-transplant lymphoproliferative disorder (PTLD) (8.9% each). In males, the most common cancers were native kidney cancer (16.4%), lung cancer (15.7%) and prostate cancer (14%). During the study period, among KTRs who developed solid organ malignancy, NMSC was diagnosed in 7.3% of recipients. The average time of occurrence of malignant tumors was 84.5 months/7 years after kidney transplantation (KTx), and most cancers developed in the range of 1-5 years (33.6%) and 5-10 years (34.42%) after KTx. Nearly half (48.8%) of patients died due to cancer.
Conclusions: Similarly to the general population, the most common cancers among KTRs included breast and prostate cancer, as well as colorectal and lung cancer. Attention should be paid to the extremely frequent occurrence of native kidney and lymphatic system cancers in this group of KTRs. The frequent occurrence of cancer in KTRs requires systematic screening in this population.
Keywords: cancer; kidney recipients; kidney transplant; malignacies; oncology in transplantation.
Copyright © 2025 Komorowska-Jagielska, Dębska-Ślizień, Kolonko, Heleniak, Ruszkowski, Czarnacka, Imko-Walczuk, Biedunkiewicz, Bułło-Piontecka, Bzoma, Chamienia, Gołębiewska, Konopa, Król, Lichodziejewska-Niemierko, Rutkowski, Tarasewicz, Więcek and Lizakowski.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Sex and gender as predictors for allograft and patient-relevant outcomes after kidney transplantation.Cochrane Database Syst Rev. 2024 Dec 19;12(12):CD014966. doi: 10.1002/14651858.CD014966.pub2. Cochrane Database Syst Rev. 2024. PMID: 39698949
-
Experience of nine south eastern European transplant centers with testicular cancer in kidney transplant recipients.Int Urol Nephrol. 2025 Sep;57(9):2877-2883. doi: 10.1007/s11255-025-04488-0. Epub 2025 Apr 1. Int Urol Nephrol. 2025. PMID: 40167983
-
Serum and urine nucleic acid screening tests for BK polyomavirus-associated nephropathy in kidney and kidney-pancreas transplant recipients.Cochrane Database Syst Rev. 2024 Nov 28;11(11):CD014839. doi: 10.1002/14651858.CD014839.pub2. Cochrane Database Syst Rev. 2024. PMID: 39606952
-
Synbiotics, prebiotics and probiotics for solid organ transplant recipients.Cochrane Database Syst Rev. 2022 Sep 20;9(9):CD014804. doi: 10.1002/14651858.CD014804.pub2. Cochrane Database Syst Rev. 2022. PMID: 36126902 Free PMC article.
-
Squamous and basal skin cancers in 17,207 solid organ transplant recipients: Real-world data from national health insurance database in Poland.Adv Clin Exp Med. 2025 Jun;34(6):901-909. doi: 10.17219/acem/199653. Adv Clin Exp Med. 2025. PMID: 39912318
References
-
- Polish national cancer profiles 2023 . Available online at: www.gov.pl.
-
- Main statistical office in Poland. Available online at: www.stat.gov.pl.
-
- National Research Registry. National Institute of Oncology . Cancer in Poland 2020. Available online at: www.onkologia.org.pl.
LinkOut - more resources
Full Text Sources