

Associations of Lymphocyte Subpopulations, Related Cytokines, Clinical Phenotypes, and Outcomes in Systemic Juvenile Idiopathic Arthritis
- PMID: 40728052
- PMCID: PMC12305351
- DOI: 10.1002/acr2.70070
Associations of Lymphocyte Subpopulations, Related Cytokines, Clinical Phenotypes, and Outcomes in Systemic Juvenile Idiopathic Arthritis
Abstract
Objective: To facilitate appropriate management, we aimed to evaluate associations between lymphocyte subsets and related cytokines with clinical characteristics and treatment outcomes of patients with systemic juvenile idiopathic arthritis (sJIA).
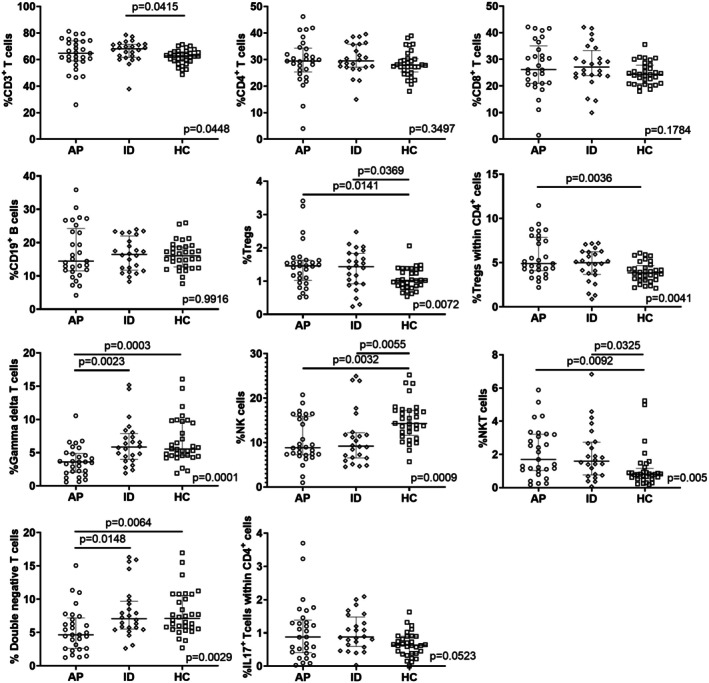
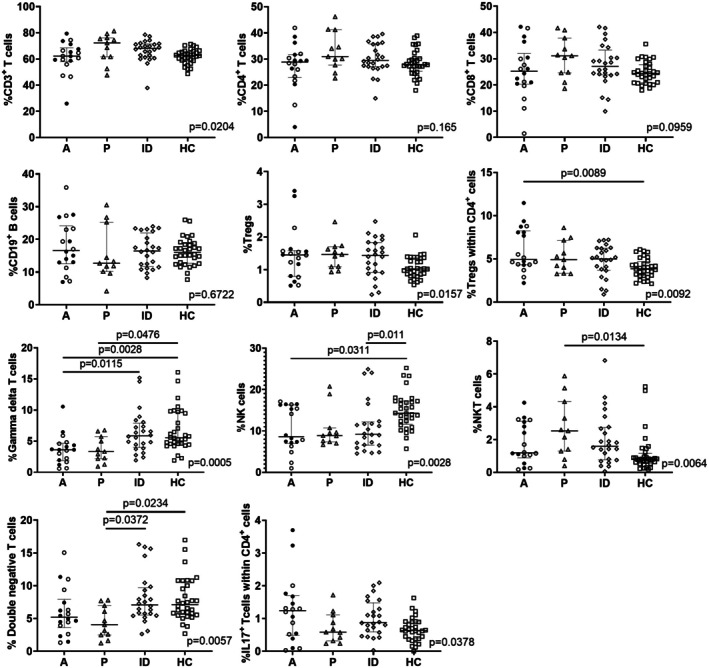
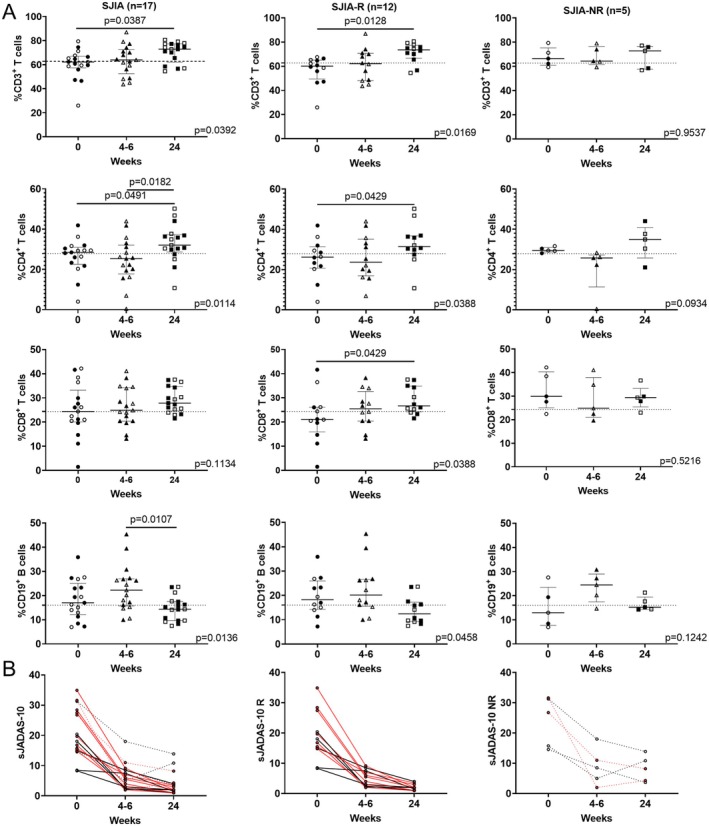
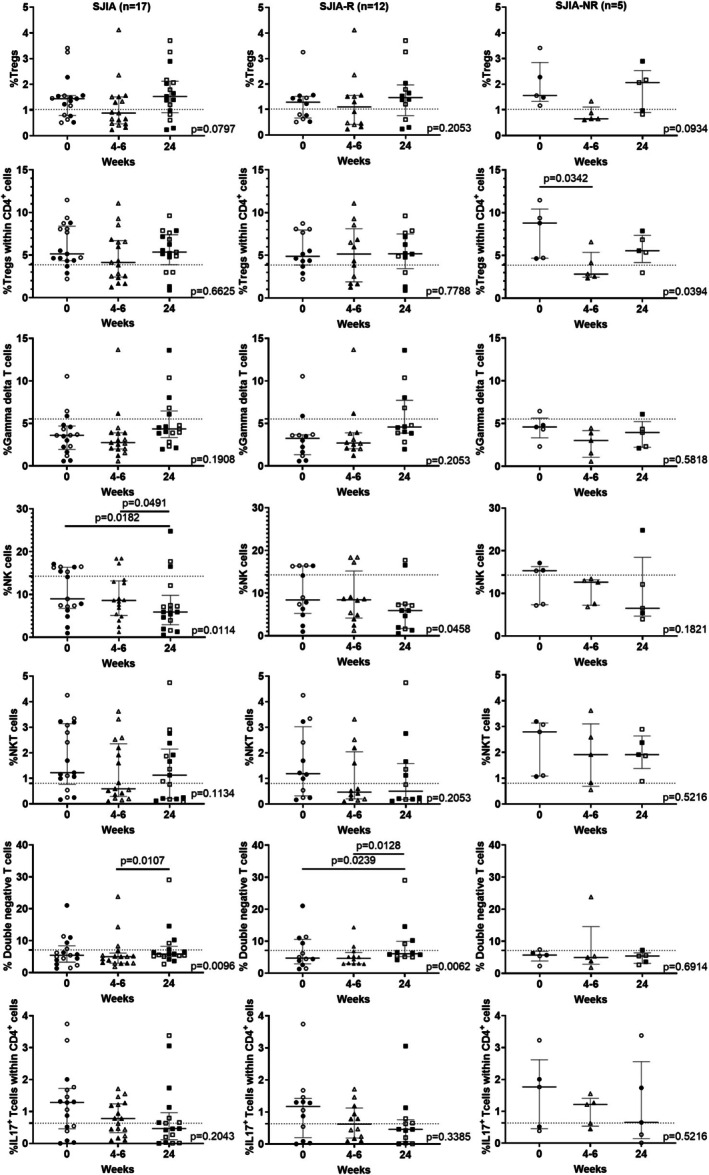
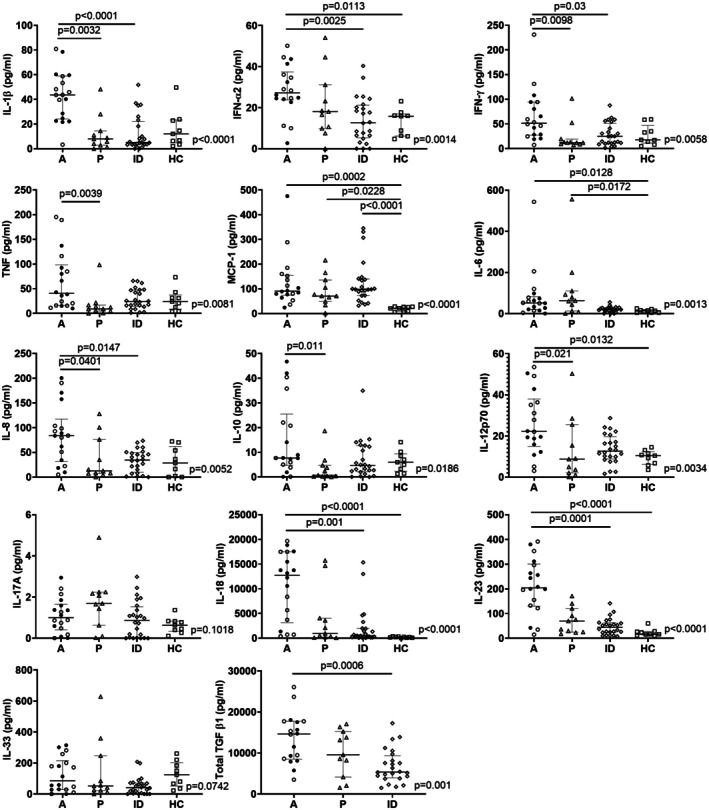
Methods: We collected blood samples from 53 patients with sJIA and evaluated the percentages of lymphocyte subsets and cytokine levels. Patients were categorized into active (n = 18), persistent (n = 11), and inactive (n = 24) sJIA groups based on clinical phenotypes. Seventeen patients with active disease provided longitudinal blood samples at 0, 4 to 6, and 24 weeks. Among these patients, 12 patients were classified as sJIA treatment responders (sJIA-R) and 5 patients were classified as sJIA treatment nonresponders (sJIA-NR). The healthy control (HC) group comprised 32 age-matched children.
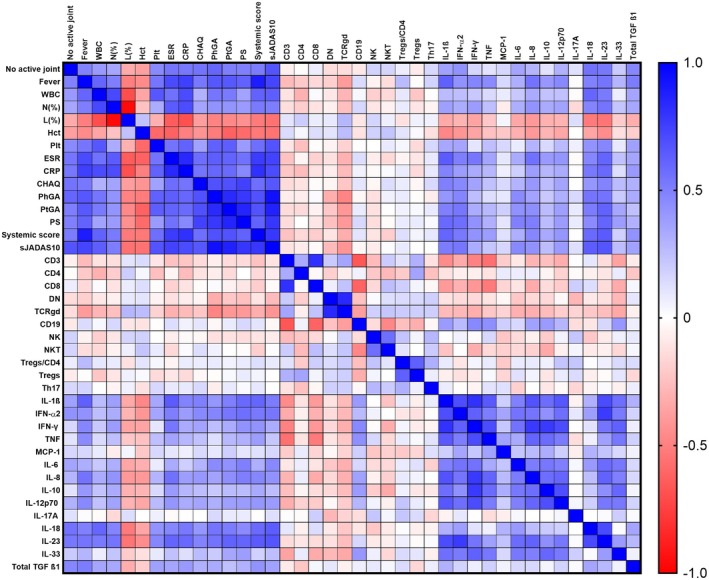
Results: Dynamic changes in lymphocyte subsets and cytokine levels were observed over time. In the longitudinal cohort, patients in the sJIA-R group showed a significant decline in proinflammatory cytokines, including interleukin-1 (IL-1), interferon-γ (IFN-γ), monocyte chemoattractant protein-1, and IL-23, along with increases in CD3+, CD4+, and CD8+ T cells. In contrast, patients in the sJIA-NR group had persistently elevated IL-1, IL-23, and tumor necrosis factor levels and natural killer (NK) T cell percentages. Despite clinical improvement, IL-18 and IFN-γ levels remained elevated compared to HCs throughout the 24-week follow-up. Analysis of minor lymphocyte subsets revealed low NK and gamma delta (γδ) T cell percentages during active disease and follow-up. Notably, IL-23 levels and γδ T cell percentages were significantly associated with several disease activity parameters.
Conclusion: Patients with sJIA exhibit altered lymphocyte subsets and inflammatory mediator production during the disease course, which may assist in identifying treatment responders and guiding therapeutic strategies. This study investigated associations of lymphocyte subpopulations, related cytokines, clinical phenotypes, and outcomes in systemic juvenile idiopathic (sJIA). Low percentages of NK and γδ-T cells were observed in patients with sJIA, particularly during active disease, compared to healthy controls. Persistent elevations in IL-1, IL-23, TNF, and NK T cell percentage were associated with poor treatment response.
© 2025 The Author(s). ACR Open Rheumatology published by Wiley Periodicals LLC on behalf of American College of Rheumatology.
Figures
References
-
- Schulert GS, Kessel C. Molecular pathways in the pathogenesis of systemic juvenile idiopathic arthritis. Rheum Dis Clin North Am 2023;49(4):895–911. - PubMed
-
- Ombrello MJ, Arthur VL, Remmers EF, et al; British Society of Pediatric and Adolescent Rheumatology (BSPAR) Study Group, Inception Cohort of Newly Diagnosed Patients with Juvenile Idiopathic Arthritis (ICON‐JIA) Study Group, Childhood Arthritis Prospective Study (CAPS) Group, Randomized Placebo Phase Study of Rilonacept in sJIA (RAPPORT) Investigators, Sparks‐Childhood Arthritis Response to Medication Study (CHARMS) Group, Biologically Based Outcome Predictors in JIA (BBOP) Group. Genetic architecture distinguishes systemic juvenile idiopathic arthritis from other forms of juvenile idiopathic arthritis: clinical and therapeutic implications. Ann Rheum Dis 2017;76(5):906–913. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
