

Radiologic evidence supporting pectoral nerve involvement in perineural spread of breast cancer to the brachial plexus
- PMID: 40728544
- PMCID: PMC12307539
- DOI: 10.1007/s00701-025-06615-3
Radiologic evidence supporting pectoral nerve involvement in perineural spread of breast cancer to the brachial plexus
Abstract
Objective: Perineural spread (PNS) of breast carcinoma to the brachial plexus is rare. This study investigates the radiologic features supporting the medial and lateral pectoral nerves (MPN and LPN, respectively) as pathways for PNS of breast cancer to the brachial plexus.
Methods: We reviewed 19 patients with biopsy-proven PNS of breast carcinoma to the brachial plexus. All available MRI and 18F-FDG PET/CT studies were re-evaluated by a musculoskeletal radiologist with expertise in PNS. Imaging features of interest included pectoralis major and minor muscle MRI signal abnormality, abnormal FDG activity, and atrophy; FDG avidity within or along the course of the pectoral nerves; and extent of brachial plexus involvement on MRI and 18F-FDG PET/CT. Demographic and clinical data were also collected.
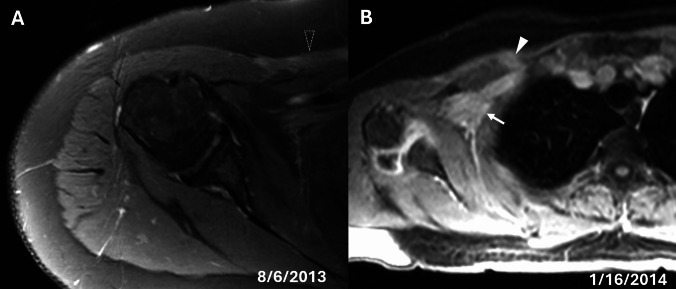
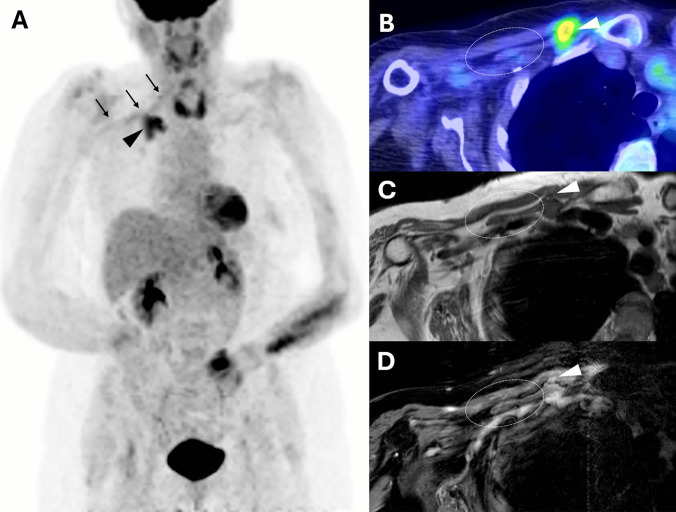
Results: All 19 patients had MRI and 18F-FDG PET/CT scans. Six patients showed clear radiologic evidence of PNS via the pectoral nerves. All six patients demonstrated abnormal MRI signal or enhancement in both the pectoralis major and minor muscles and increased FDG uptake was present in the pectoralis major in 4/6 patients and pectoralis minor in 5/6 patients. Five patients demonstrated atrophy of both the pectoralis major and minor muscles. Increased FDG uptake was noted along the LPN in five patients and the MPN in four. All exhibited brachial plexus enhancement on MRI and increased FDG uptake on PET/CT, supporting contiguous spread from the pectoral nerves.
Conclusion: This study provides radiologic support for the MPN and LPN as a potential pathway for PNS of breast cancer to the brachial plexus. Pectoralis major/minor muscle atrophy, abnormal MRI signal or enhancement, and increased FDG activity within the pectoral muscles and/or along the pectoral nerves may serve as early, non-invasive imaging markers of this process, with potential implications for diagnosis and management.
Keywords: Brachial plexus; Breast cancer; MRI; Pectoral nerves; Perineural spread.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests.: The authors declare no competing interests.
Figures




Similar articles
-
Brachial plexopathy due to perineural tumor spread: a retrospective single-center experience of clinical manifestations, diagnosis, treatments, and outcomes.Acta Neurochir (Wien). 2024 Dec 2;166(1):490. doi: 10.1007/s00701-024-06381-8. Acta Neurochir (Wien). 2024. PMID: 39621168
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article.
-
The value of FDG positron emission tomography/computerised tomography (PET/CT) in pre-operative staging of colorectal cancer: a systematic review and economic evaluation.Health Technol Assess. 2011 Sep;15(35):1-192, iii-iv. doi: 10.3310/hta15350. Health Technol Assess. 2011. PMID: 21958472 Free PMC article.
-
PET-CT for assessing mediastinal lymph node involvement in patients with suspected resectable non-small cell lung cancer.Cochrane Database Syst Rev. 2014 Nov 13;2014(11):CD009519. doi: 10.1002/14651858.CD009519.pub2. Cochrane Database Syst Rev. 2014. PMID: 25393718 Free PMC article.
-
¹⁸F-FDG PET/CT: a review of diagnostic and prognostic features in multiple myeloma and related disorders.Clin Exp Med. 2015 Feb;15(1):1-18. doi: 10.1007/s10238-014-0308-3. Epub 2014 Sep 14. Clin Exp Med. 2015. PMID: 25218739
References
-
- Mamtani A, Andrea V Barrio Md (2025) Updates in surgical management of the axilla. Oncology (Williston Park) 39(2):70–75 - PubMed
-
- Balamucki CJ, Mancuso AA, Amdur RJ, Kirwan JM, Morris CG, Flowers FP, Stoer CB, Cognetta AB, Mendenhall WM (2012) Skin carcinoma of the head and neck with perineural invasion. Am J Otolaryngol 33(4):447–454 - PubMed
-
- Belmonte R, Monleon S, Bofill N, Alvarado ML, Espadaler J, Royo I (2015) Long thoracic nerve injury in breast cancer patients treated with axillary lymph node dissection. Support Care Cancer 23(1):169–175 - PubMed
-
- Cao W, Howe BM, Ramanathan S, Rhodes NG, Korfiatis P, Amrami KK, Spinner RJ, Kline TL (2024) Non-traumatic brachial plexopathy identification from routine MRIs: Retrospective studies with deep learning networks. Eur J Radiol 181(111744):111744 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
