

Low-dose ultrahigh-resolution PCCT enhances subsolid nodule characterization
- PMID: 40728552
- PMCID: PMC12367857
- DOI: 10.1007/s11547-025-02057-0
Low-dose ultrahigh-resolution PCCT enhances subsolid nodule characterization
Abstract
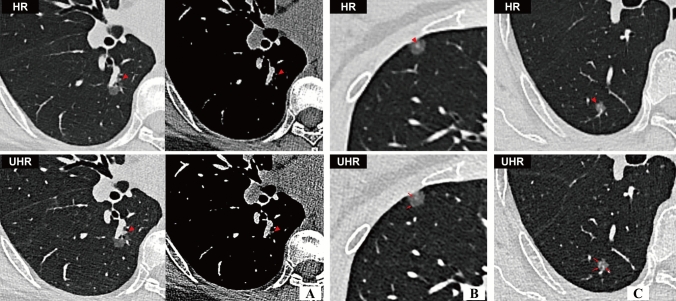
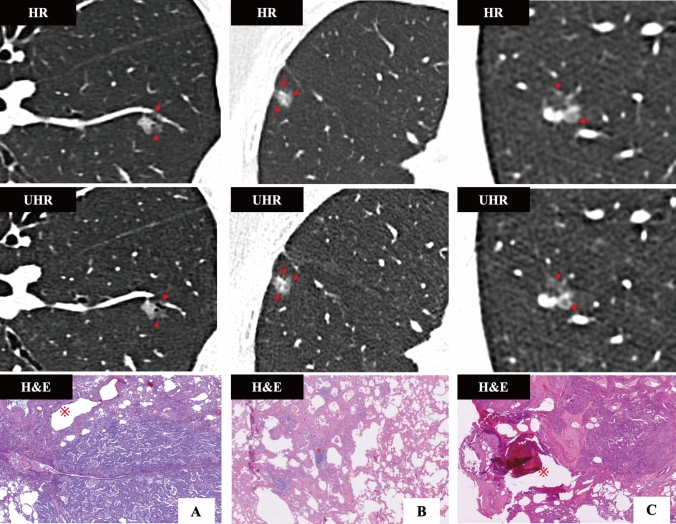
Purpose: To characterize invasion-associated CT features in pulmonary subsolid nodules using low-dose ultrahigh-resolution (UHR) photon-counting CT (PCCT) images and evaluate UHR's diagnostic superiority over standard high-resolution (HR) images.
Methods: Patients with subsolid lung adenocarcinoma were recruited for chest scan on PCCT to obtain UHR and standard HR images between November 2023 and May 2024. Nodule characteristics were visually assessed and histogram features were extracted from each nodule. Image quality and radiation dose at previous energy-integrating detector CT (EID-CT) of 30 patients were compared with those of PCCT. Differences between UHR and standard HR, PCCT and EID-CT were compared using paired McNemar-test or paired Wilcox-test.
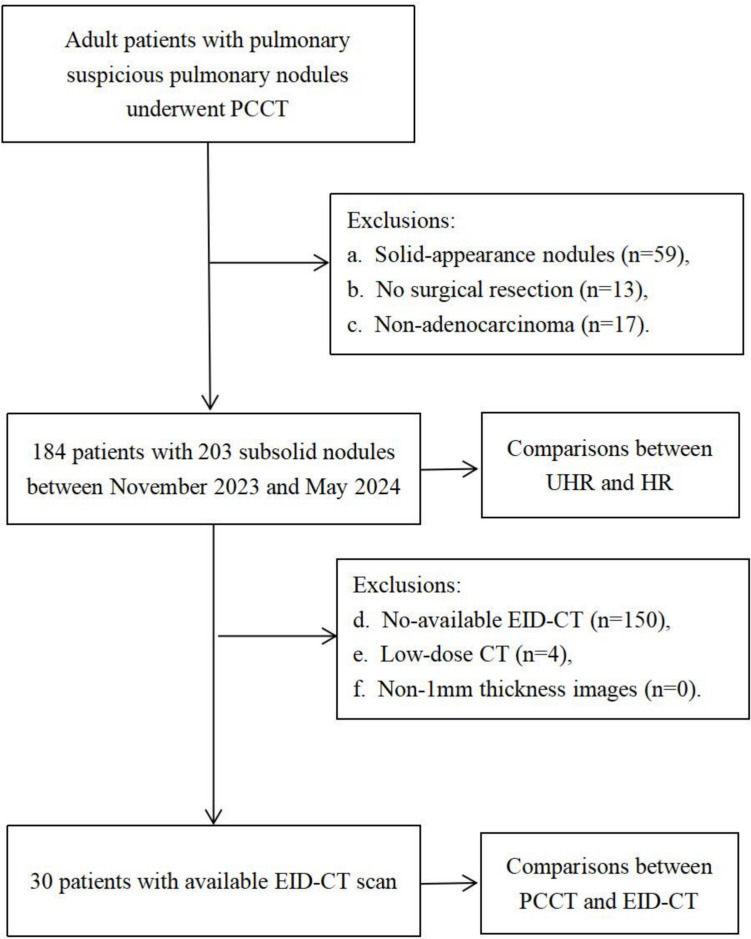
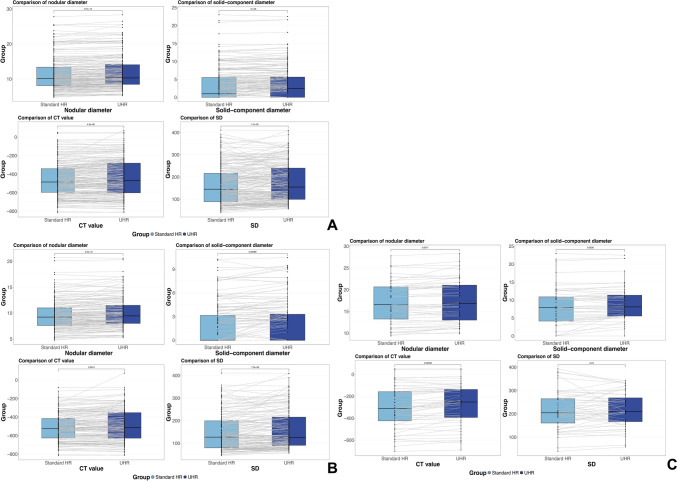
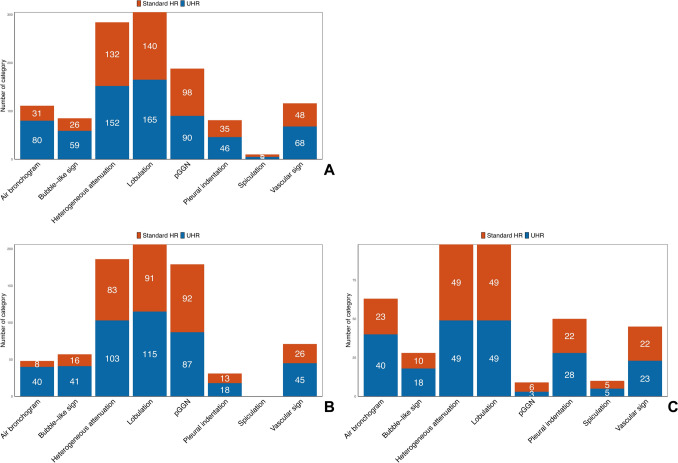
Results: One hundred and eighty-four patients with 203 subsolid nodules were collected including 77 precursors, 77 minimally invasive adenocarcinoma (MIA) and 49 IA. UHR significantly outperformed standard HR in revealing CT findings including larger nodular diameter and solid-component diameter, more frequency of heterogeneous attenuation, lobulation, bubble-like sign, air bronchogram, pleural indentation and vascular sign (all P < 0.05). Additionally, UHR images exhibited significantly greater value in histogram-derived parameters compared to standard HR images (all P < 0.05), except for "Median," "Minimum." Furthermore, the radiation dose in PCCT was half of that in EID-CT (effective dose: 1.32 ± 0.27 vs. 3.85 ± 1.65/mSv, P < 0.001. CDTIvol: 2.97 ± 0.53 vs. 6.90 ± 2.97/mGy, P < 0.001), with image quality significantly better in PCCT.
Conclusion: The UHR protocol on PCCT provides a magnified perspective to reveal CT characteristics of invasive growth in subsolid LUAD, previously undetectable on standard HR images, achieving halved radiation dose and better image quality than EID-CT.
Keywords: Lung adenocarcinoma; Photon-counting CT; Subsolid nodules; Ultrahigh resolution.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors have no relevant financial or non-financial interests to disclose. Ethical approval: This study was approved by the ethical review board of Ruijin Hospital Affiliated to Shanghai Jiaotong University Medical School (AF0406/14.0/2023–03-01). Consent to participate: Written informed consent was waived by the Institutional Review Board. Consent for publication: The authors affirm that human research participants provided informed consent for publication of the images in Figs. 5A–C and 6A–C.
Figures
References
-
- R Fujikawa Y Muraoka J Kashima Y Yoshida K Ito H Watanabe M Kusumoto SI Watanabe Y Yatabe 2022 Clinicopathologic and genotypic features of lung adenocarcinoma characterized by the international association for the study of lung cancer grading system J Thorac Oncol 17 5 700 707 10.1016/j.jtho.2022.02.005 - DOI - PubMed
-
- WD Travis E Brambilla M Noguchi AG Nicholson KR Geisinger Y Yatabe DG Beer CA Powell GJ Riely PE Schil Van K Garg JH Austin H Asamura VW Rusch FR Hirsch G Scagliotti T Mitsudomi RM Huber Y Ishikawa J Jett M Sanchez-Cespedes JP Sculier T Takahashi M Tsuboi J Vansteenkiste I Wistuba PC Yang D Aberle C Brambilla D Flieder W Franklin A Gazdar M Gould P Hasleton D Henderson B Johnson D Johnson K Kerr K Kuriyama JS Lee VA Miller I Petersen V Roggli R Rosell N Saijo E Thunnissen M Tsao D Yankelewitz 2011 International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma J Thorac Oncol 6 2 244 285 10.1097/JTO.0b013e318206a221 - DOI - PMC - PubMed
-
- J Zhang J Wu Q Tan L Zhu W Gao 2013 Why do pathological stage IA lung adenocarcinomas vary from prognosis?: a clinicopathologic study of 176 patients with pathological stage IA lung adenocarcinoma based on the IASLC/ATS/ERS classification J Thorac Oncol 8 9 1196 1202 10.1097/JTO.0b013e31829f09a7 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
