

Implementing clinical guidelines for gestational weight gain care: a novel application of best-worst scaling to prioritise barriers
- PMID: 40731004
- PMCID: PMC12308902
- DOI: 10.1186/s12913-025-13108-7
Implementing clinical guidelines for gestational weight gain care: a novel application of best-worst scaling to prioritise barriers
Abstract
Background: Antenatal clinical guidelines recommending the provision of care for gestational weight gain (GWG) are not routinely delivered by antenatal care providers (ACPs). Determining barriers to such care delivery can inform the development of targeted strategies to improve implementation. However, no previous studies have identified which barriers are most important.
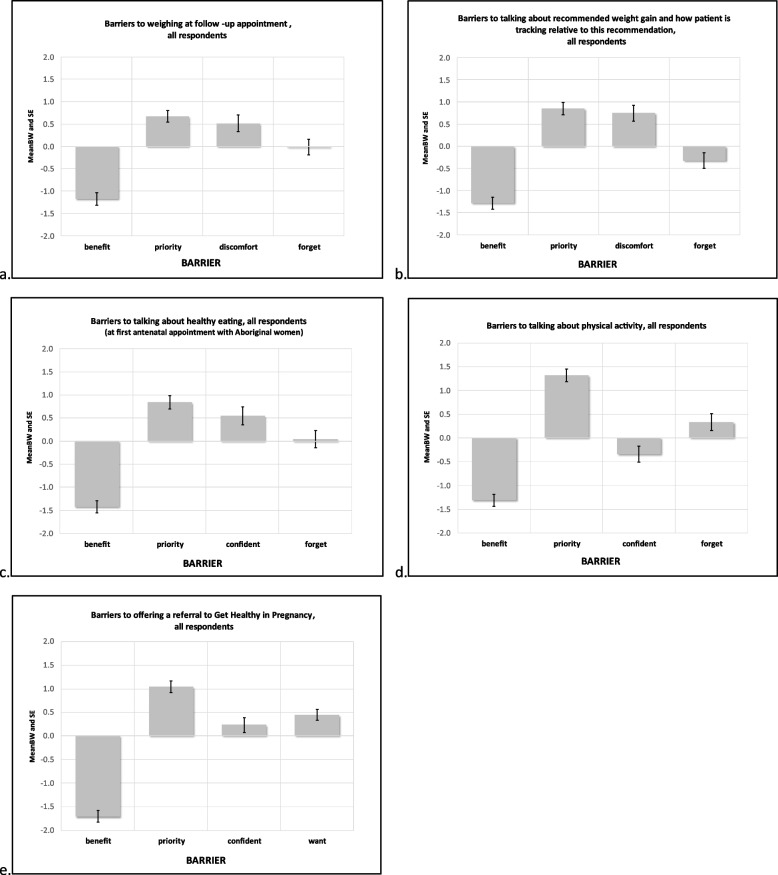
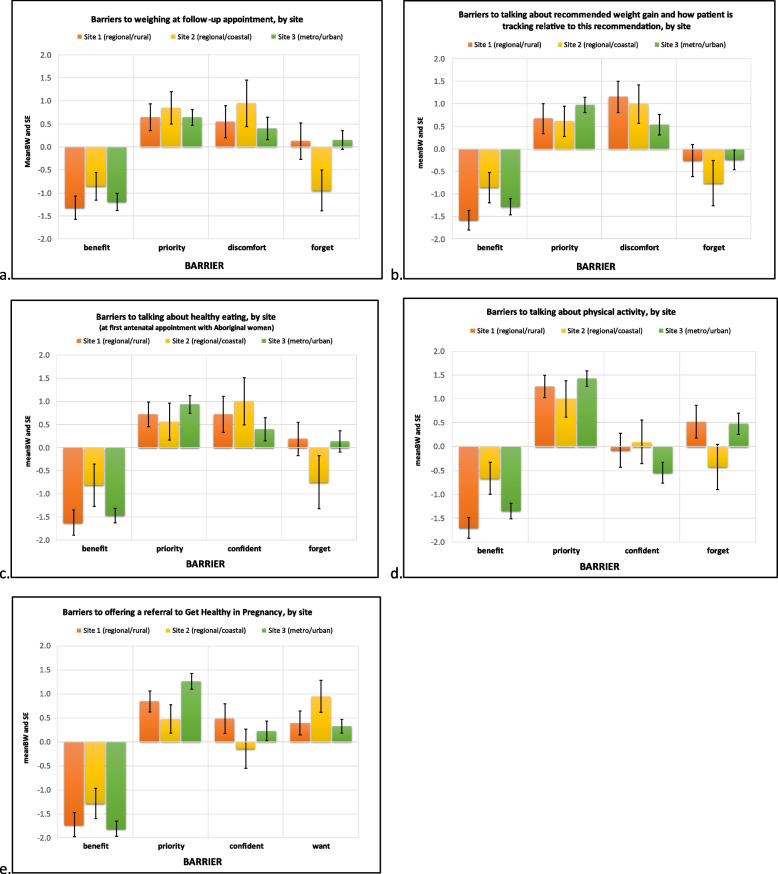
Methods: A best-worst scaling (BWS) survey was developed to estimate the magnitude and rank the importance of barriers to the delivery of recommended GWG care. The survey was conducted between December 2020 and November 2021 with ACPs (medical, midwifery, and Aboriginal health workers) who provided care in public maternity services within three sites in New South Wales, Australia. ACPs were asked to select which of four barriers were most and least likely to inhibit five recommended GWG care practices (assessment of GWG; advice on GWG, diet and physical activity; and referral to specialist GWG services). Rankings of barriers were determined through choice frequency analysis for ACPs at each site.
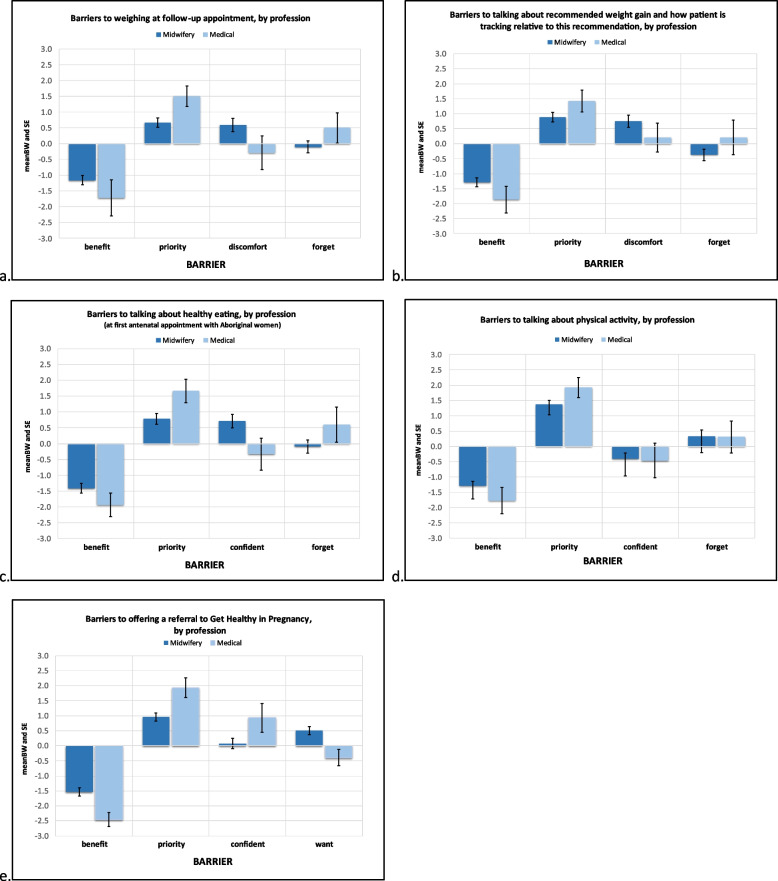
Results: A total of 143 ACPs completed the survey (64.4% response rate). For each of the five recommended GWG care practices, the most important barrier across all health sites and for both midwives and medical ACPs was 'compared to other aspects of my job, the guideline care is not a high priority.' There was some variation in the importance of barriers between sites. Across all sites, medical staff were more likely than midwives to report 'I forget' as a barrier to weighing and providing weight tracking and dietary advice and 'I don't feel confident (providing this GWG care practice)' as a barrier to providing referrals to a specialist GWG service.
Conclusions: Best-worst scaling was a valuable method to rank the influence of barriers and to prioritise site-specific and profession-based barriers to ACP provision of guideline-recommended care for GWG. Not all barriers were equally important, and this 'hierarchy' differed across ACPs and sites. Implementation strategies should be developed to address the highest priority barriers, tailored to site and professional needs.
Trial registration: Australian and New Zealand Clinical Trials Registry, ACTRN12621000054819 (22/01/2021). http://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=380680&isReview=true.
Keywords: Antenatal care; Barriers; Best–worst scaling; Gestational weight gain; Implementation; Prioritisation.
© 2025. Crown.
Conflict of interest statement
Declarations. Ethics Approval and Consent to Participate: As this study involved human participants, the conduct of the research was performed in compliance with the Declaration of Helsinki. The study, including approval of consent methods and experimental methods, was approved and conducted in accordance with the relevant ethics institutions, including the Hunter New England Human Research Ethics Committee (16/10/19/5.15) and the University of Newcastle Human Research Ethics Committee (H-2016–0422). All respondents participating in data collection were fully informed of the purpose and procedures of the study and provided informed consent to participate prior to survey commencement. Respondents could decline participation and withdraw consent at any time. All participants were assured of the confidentiality of information provided. Consent for publication: Not applicable. Competing Interests: EF, JW, JH, JD, MF, CP, LW and MK receive salary support from Hunter New England Clinical Services Nursing and Midwifery, which contributes funding to the research project. JH is supported by the Prevention Research Support Program, funded by the New South Wales Ministry of Health. All other authors declare that they have no competing interests..
Figures
References
-
- National Research Council (U.S.). Committee to Reexamine I.O.M. Pregnancy Weight Guidelines. Weight Gain During Pregnancy: Reexamining the Guidelines. Rasmussen KM, Yaktine AL, editors. Washington (D.C.): The National Academies Press (US); 2009. 10.17226/12584. PMID: 20669500. - PubMed
-
- Davis-Moss R, Hofferth S. Inadequate Gestational Weight Gain and Malnutrition-Related Causes of Infant Death. J Pregnancy Reprod. 2018;2.
-
- Rogozińska E, Zamora J, Marlin N, Betrán AP, Astrup A, Bogaerts A, et al. Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: analysis using individual participant data from randomised trials. BMC Pregnancy Childbirth. 2019;19(1):322. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
