

The Relationship Between Chest Wall Muscle Thickness, Pulmonary Function, and Prognostic Markers in Idiopathic Pulmonary Fibrosis
- PMID: 40731811
- PMCID: PMC12298751
- DOI: 10.3390/medicina61071181
The Relationship Between Chest Wall Muscle Thickness, Pulmonary Function, and Prognostic Markers in Idiopathic Pulmonary Fibrosis
Abstract
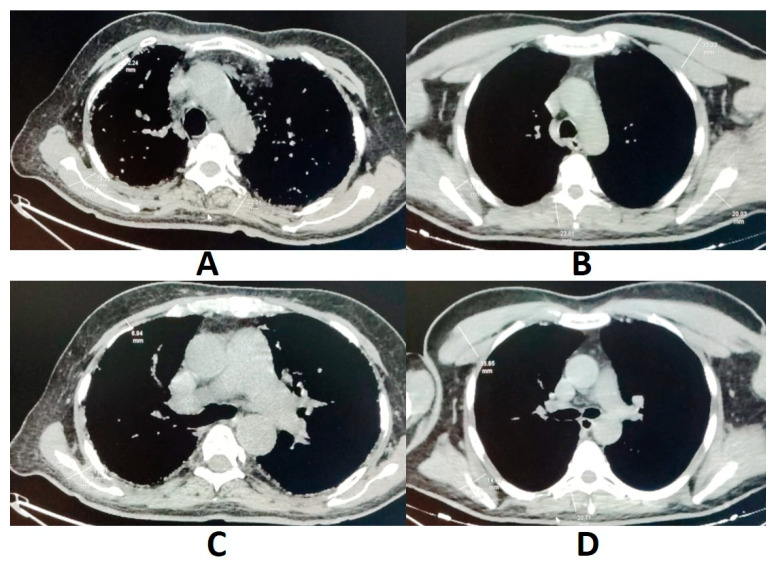
Background and Objectives: Idiopathic pulmonary fibrosis (IPF) is a specific form of chronic, progressive interstitial lung disease with an unknown etiology. It is often accompanied by skeletal muscle mass loss. Chest wall muscles play a crucial role in respiratory movements and form part of the skeletal muscles. The aim of this study is to evaluate the relationship between chest wall muscle thickness and pulmonary function test (PFT) results, as well as other prognostic markers, in patients with IPF. Materials and Methods: A retrospective analysis was conducted on 108 patients diagnosed with IPF and 53 control subjects. Chest wall muscle thickness was measured on thoracic computed tomography (CT) images at specific anatomical levels. PFT parameters, the Gender-Age-Physiology (GAP) index, number of acute exacerbations, and mortality data were evaluated in relation to muscle thickness. Results: IPF patients had significantly reduced thickness in the bilateral external scapular muscles at both the aortic and pulmonary trunk levels compared to controls. Bilateral pectoral muscle thickness at the aortic level was positively correlated with forced vital capacity (FVC) and negatively correlated with the number of exacerbations. Internal scapular muscle thickness at the aortic level showed a significant positive correlation with diffusion capacity of the lung for carbon monoxide (DLCO) and a negative correlation with both GAP scores and exacerbation frequency. External scapular muscle thickness at the pulmonary trunk level was positively associated with PFT parameters and inversely correlated with the GAP index, exacerbations, and mortality. Conclusions: In patients with IPF, the bilateral external scapular muscle thickness at the aortic and pulmonary trunk levels was significantly reduced compared to controls. Significant associations were found between some chest wall muscle thicknesses and the GAP index, pulmonary function, acute exacerbations, and mortality, underscoring the prognostic value of baseline muscle measurements. Measurement of chest wall muscle thickness using routine thoracic CT scans may offer additional prognostic value in IPF. Incorporating this parameter into clinical evaluation may help identify patients who could benefit from supportive interventions, such as nutritional therapy or pulmonary rehabilitation.
Keywords: chest wall muscle mass; idiopathic pulmonary fibrosis; prognosis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Long-Term Air Pollution Exposure and Severity of Idiopathic Pulmonary Fibrosis: Data from the Idiopathic Pulmonary Fibrosis Prospective Outcomes (IPF-PRO) Registry.Ann Am Thorac Soc. 2025 Mar;22(3):378-386. doi: 10.1513/AnnalsATS.202404-382OC. Ann Am Thorac Soc. 2025. PMID: 39531618
-
Conventional chest physiotherapy compared to other airway clearance techniques for cystic fibrosis.Cochrane Database Syst Rev. 2023 May 5;5(5):CD002011. doi: 10.1002/14651858.CD002011.pub3. Cochrane Database Syst Rev. 2023. PMID: 37144842 Free PMC article.
-
Dynamics of interstitial lung disease following immunosuppressive treatment differ between antisynthetase syndrome and systemic sclerosis.Ther Adv Respir Dis. 2025 Jan-Dec;19:17534666251336896. doi: 10.1177/17534666251336896. Epub 2025 May 8. Ther Adv Respir Dis. 2025. PMID: 40337907 Free PMC article.
-
Bronchoscopy-guided antimicrobial therapy for cystic fibrosis.Cochrane Database Syst Rev. 2024 May 3;5(5):CD009530. doi: 10.1002/14651858.CD009530.pub5. Cochrane Database Syst Rev. 2024. PMID: 38700027 Free PMC article.
-
Intravenous antibiotics for pulmonary exacerbations in people with cystic fibrosis.Cochrane Database Syst Rev. 2025 Jan 20;1(1):CD009730. doi: 10.1002/14651858.CD009730.pub3. Cochrane Database Syst Rev. 2025. PMID: 39831540
References
-
- Raghu G., Remy-Jardin M., Richeldi L., Thomson C.C., Inoue Y., Johkoh T., Kreuter M., Lynch D.A., Maher T.M., Martinez F.J., et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: An official ATS/ERS/JRS/ALAT clinical practice guideline. Am. J. Respir. Crit. Care Med. 2022;205:e18–e47. doi: 10.1164/rccm.202202-0399ST. - DOI - PMC - PubMed
-
- Ruaro B., Pozzan R., Confalonieri P., Tavano S., Hughes M., Matucci Cerinic M., Baratella E., Zanatta E., Lerda S., Geri P., et al. Gastroesophageal Reflux Disease in Idiopathic Pulmonary Fibrosis: Viewer or Actor? To Treat or Not to Treat? Pharmaceuticals. 2022;15:1033. doi: 10.3390/ph15081033. - DOI - PMC - PubMed
-
- Monteleone G., Bergantini L., D’Alessandro M., Pianigiani T., Simonetti J., Iovene B., Varone F., Sgalla G., Richeldi L., Bargagli E., et al. The management of Familial Pulmonary Fibrosis in different medical settings: Where does that leave us? An Italian nationwide survey. Sarcoidosis Vasc. Diffus. Lung Dis. 2024;41:e2024047. doi: 10.36141/svdld.v41i3.15744. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
