

Diagnostic Accuracy of Non-Radiologist-Performed Ultrasound for Diagnosing Acute Appendicitis in Pediatric Patients: A Systematic Review and Meta-Analysis
- PMID: 40731937
- PMCID: PMC12299215
- DOI: 10.3390/medicina61071308
Diagnostic Accuracy of Non-Radiologist-Performed Ultrasound for Diagnosing Acute Appendicitis in Pediatric Patients: A Systematic Review and Meta-Analysis
Abstract
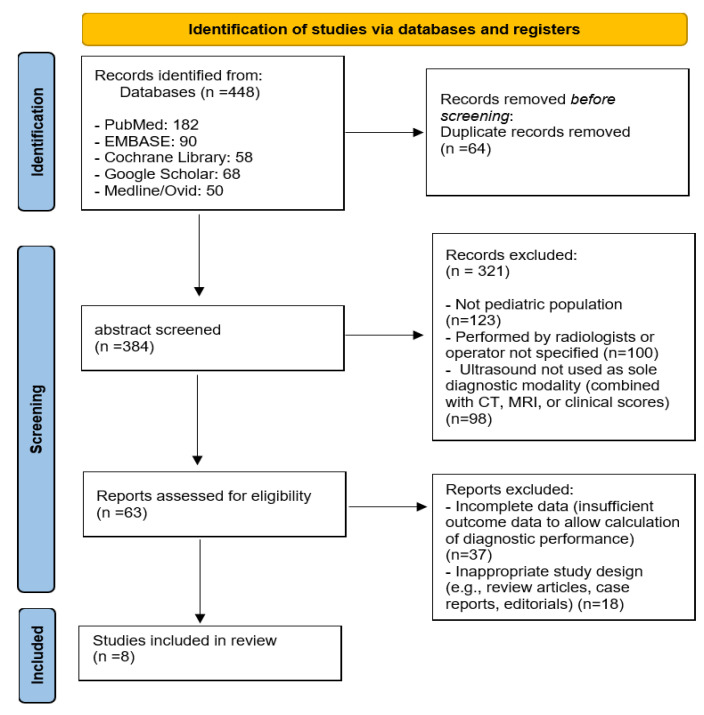
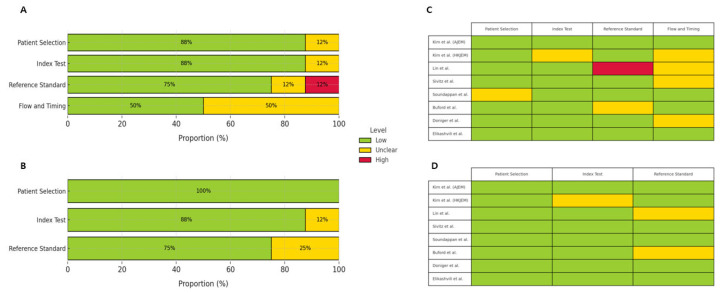
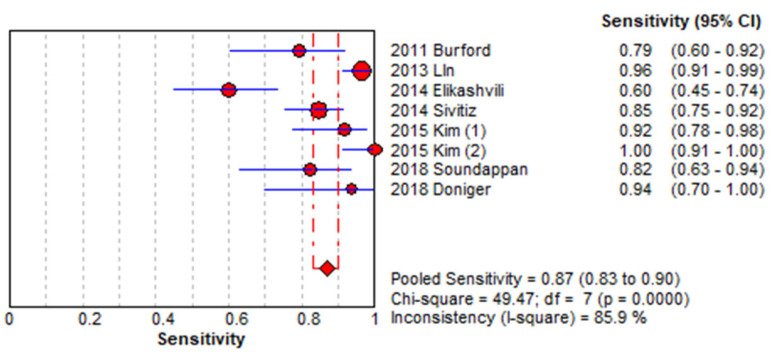
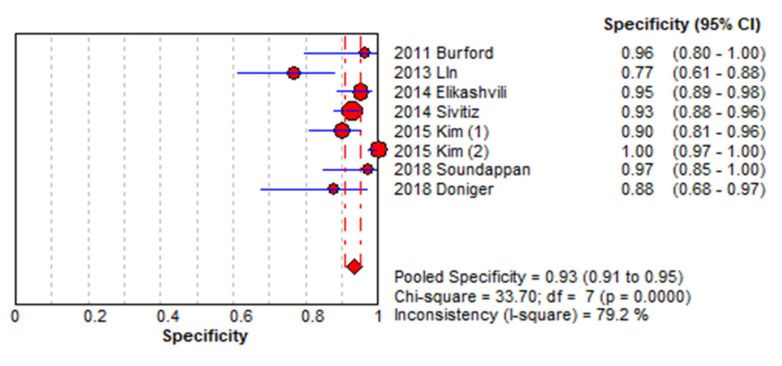
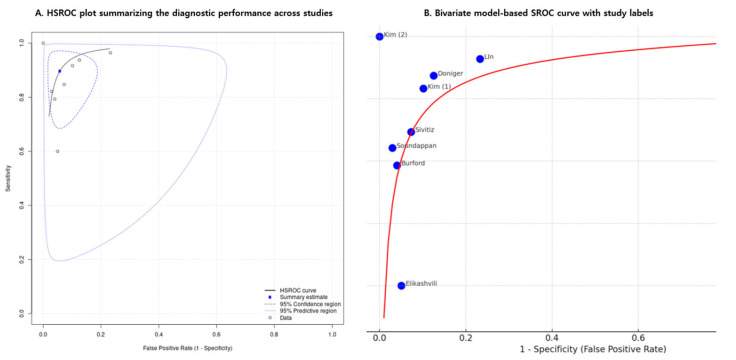
Background and Objectives: Acute appendicitis is a common cause of abdominal pain requiring surgery in pediatric patients. Given concerns regarding radiation exposure from computed tomography (CT), ultrasound (US) has become the first-line diagnostic modality. In many emergency and resource-limited settings, non-radiologist physicians often perform these examinations. This study aimed to evaluate the diagnostic accuracy of a non-radiologist-performed ultrasound in detecting acute appendicitis in children. Materials and Methods: We conducted a systematic review and meta-analysis according to the PRISMA guidelines. The literature was searched across PubMed, Ovid MEDLINE, EMBASE, the Cochrane Library, and Google Scholar through June 2024. Studies reporting on the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of non-radiologist-performed ultrasounds in pediatric appendicitis were included. Study quality was assessed using the QUADAS-2 tool, and a bivariate random-effects model was used for statistical analysis. Results: Eight studies, with a total of 1006 pediatric patients, were included. The pooled sensitivity and specificity were 0.87 (95% CI, 0.83-0.90) and 0.93 (95% CI, 0.91-0.95), respectively. The area under the SROC curve was 0.783 (95% CI, 0.708-0.853), suggesting moderate-to-good diagnostic accuracy. Substantial heterogeneity was observed across studies, possibly due to differences in operator training and ultrasound techniques. Conclusions: Non-radiologist-performed ultrasound demonstrates moderate-to-good diagnostic accuracy in identifying pediatric appendicitis. These findings support its implementation in emergency or resource-constrained settings and suggest that incorporating structured ultrasound training for non-radiologists may improve timely diagnosis and optimize clinical decision-making in pediatric emergency care.
Keywords: appendicitis; child; systematic review; ultrasonography.
Conflict of interest statement
The author declare no conflicts of interest.
Figures
Similar articles
-
Accuracy of Point-of-care Ultrasonography for Diagnosing Acute Appendicitis: A Systematic Review and Meta-analysis.Acad Emerg Med. 2017 Sep;24(9):1124-1136. doi: 10.1111/acem.13212. Epub 2017 Aug 21. Acad Emerg Med. 2017. PMID: 28464459
-
Diagnostic Accuracy of History, Physical Examination, Laboratory Tests, and Point-of-care Ultrasound for Pediatric Acute Appendicitis in the Emergency Department: A Systematic Review and Meta-analysis.Acad Emerg Med. 2017 May;24(5):523-551. doi: 10.1111/acem.13181. Acad Emerg Med. 2017. PMID: 28214369
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2022 May 16;5(5):CD013639. doi: 10.1002/14651858.CD013639.pub5. Cochrane Database Syst Rev. 2022. PMID: 35575286 Free PMC article.
-
Regional cerebral blood flow single photon emission computed tomography for detection of Frontotemporal dementia in people with suspected dementia.Cochrane Database Syst Rev. 2015 Jun 23;2015(6):CD010896. doi: 10.1002/14651858.CD010896.pub2. Cochrane Database Syst Rev. 2015. PMID: 26102272 Free PMC article.
-
Transabdominal ultrasound and endoscopic ultrasound for diagnosis of gallbladder polyps.Cochrane Database Syst Rev. 2018 Aug 15;8(8):CD012233. doi: 10.1002/14651858.CD012233.pub2. Cochrane Database Syst Rev. 2018. PMID: 30109701 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
