

Growing Pains and Dietary Habits in Young Athletes: A Cross-Sectional Survey
- PMID: 40733009
- PMCID: PMC12299381
- DOI: 10.3390/nu17142384
Growing Pains and Dietary Habits in Young Athletes: A Cross-Sectional Survey
Abstract
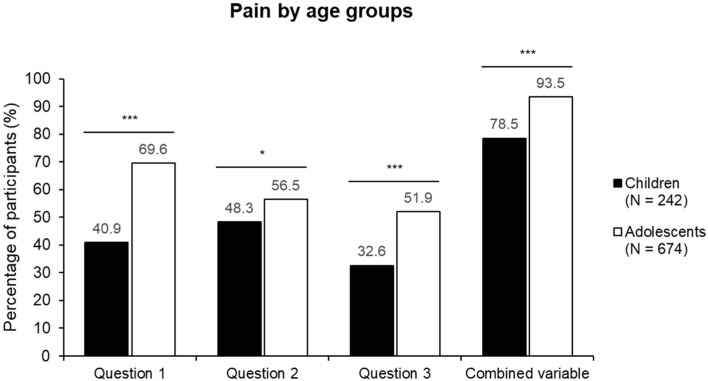
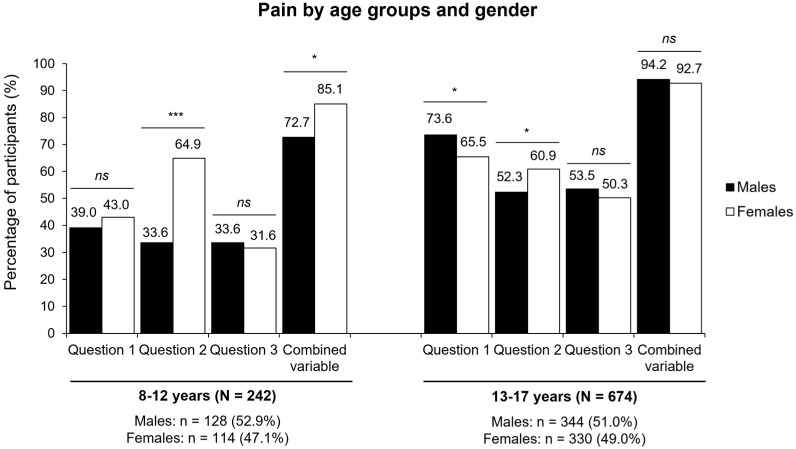
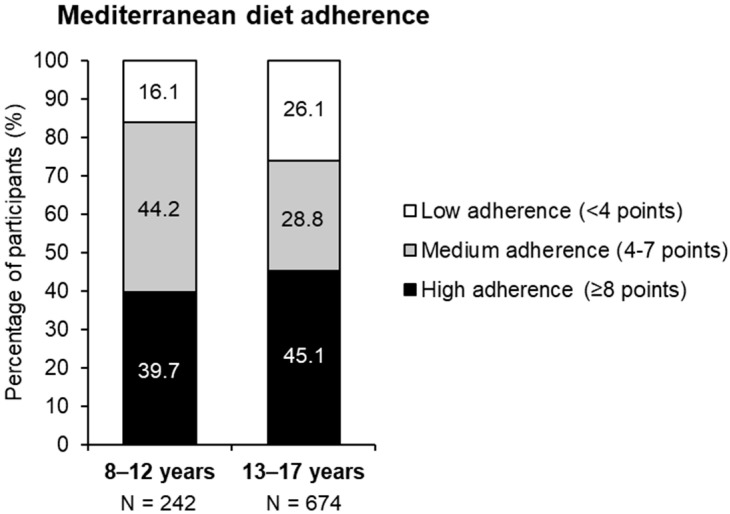
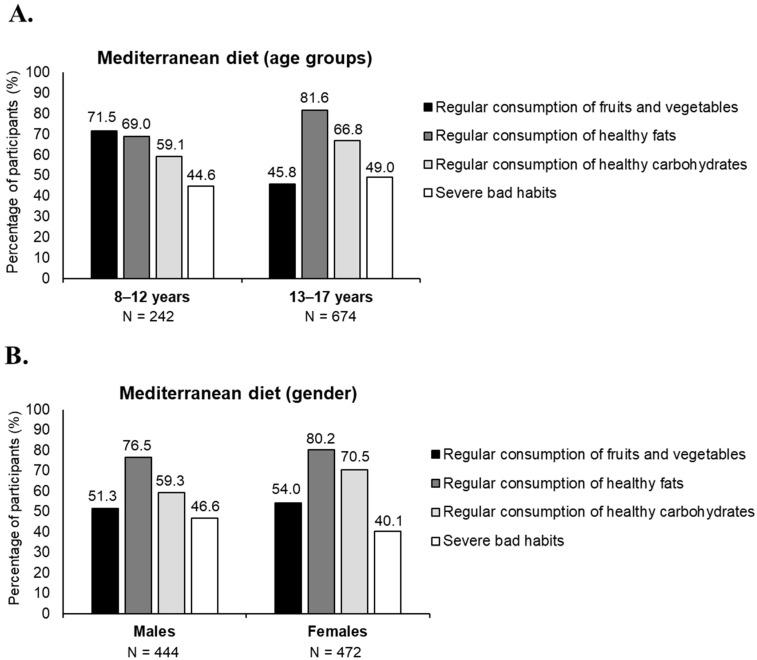
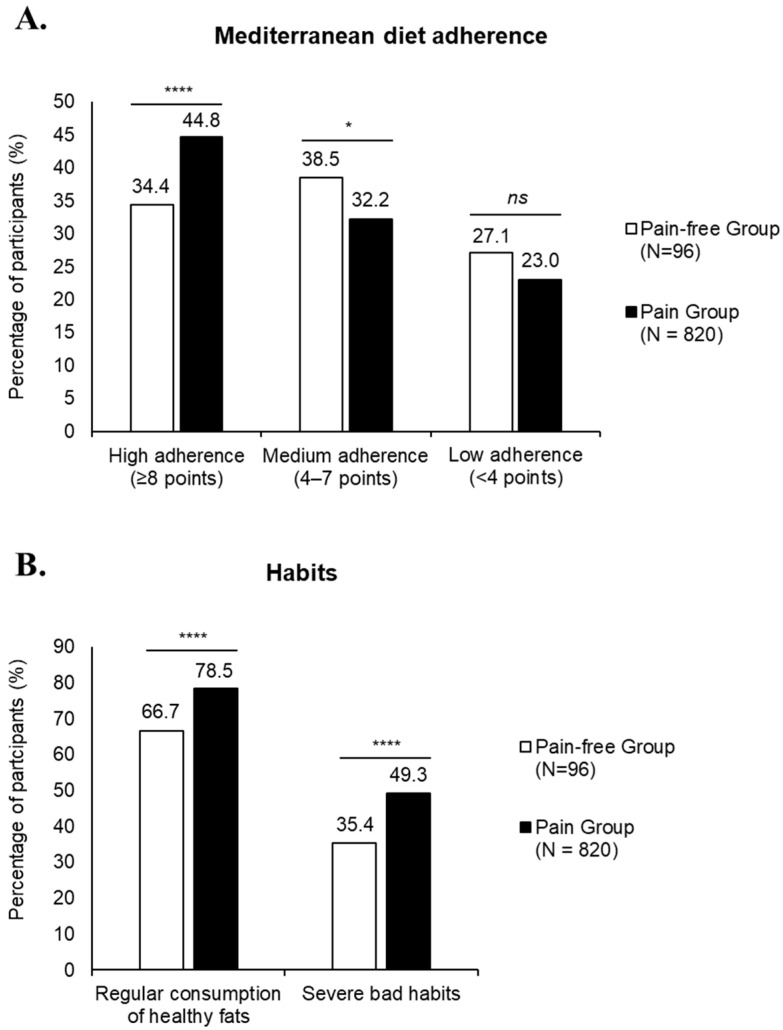
Background/Objectives: Growing pains are a common cause of recurrent limb pain in children, but their etiology remains unclear. Physical activity and nutrition are important factors for musculoskeletal health, but their specific relationship with growing pains has not been well established in young athletes. This study aimed to assess the prevalence of growing pains in child and adolescent athletes and evaluate their adherence to the Mediterranean Diet. Methods: A cross-sectional study was conducted with 916 athletes aged 8-17 years from sports academies in Alicante, Spain. Data were collected via an online survey assessing demographics, pain types, and adherence to the Mediterranean diet. Results: Self-reported pain was highly prevalent, affecting 78.5% of children and 93.5% of adolescents. Musculoskeletal and nocturnal pain increased with age, with nocturnal pain significantly more frequent in girls among children (p < 0.001). Additionally, 32.6% of children and 51.9% of adolescents had received a formal diagnosis of growing pains. Despite this, only 13.7% reported using analgesics, with no significant gender differences. Adherence to the Mediterranean diet was mostly moderate, with children reporting higher fruit and vegetable intake than adolescents, while adolescents consumed more healthy fats and carbohydrates, and participants without pain showed overall healthier dietary patterns. Conclusions: Idiopathic musculoskeletal pain is highly prevalent among young athletes, and their adherence to a healthy diet is suboptimal, challenging the assumption that physically active children maintain well-balanced diets. This underscores the importance of early nutritional education as a strategy to support musculoskeletal health and reduce pain in physically active youth.
Keywords: Mediterranean diet; dietary habits; growing pains; musculoskeletal pain.
Conflict of interest statement
M.P. and R.D.-C. are employees of Laboratorios Ordesa, S.L., the sponsor of this study. Authors C.E-A., J.A.P.T. and C.S.-L. were employed by the company Kinetic Performance S.L. The authors declare that this study received funding from Laboratorios Ordesa, S.L. None of the authors received personal compensation related to this study, and no author had any commercial or financial relationships that could be construed as a potential conflict of interest. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Figures
References
-
- Duchamp M. Maladies de la croissance. In: Levrault F.G., editor. Memoires de Médecine Practique. Jean-Frederic Lobstein; Paris, France: 1823.
-
- González B. Growing pain in children: Myth or true? Rev. Méd. Clín. Las Condes. 2009;20:892–896.
-
- Mollo Tangara J.C., Valdivie Rojas N. Dolores de crecimiento/growing pains. Cienc. Méd. 2014;17:37–42.
MeSH terms
LinkOut - more resources
Full Text Sources
