

Long-Term Effect of Semaglutide on the Glomerular Filtration Rate Slope in High-Risk Patients with Diabetic Nephropathy: Analysis in Real-World Clinical Practice
- PMID: 40733151
- PMCID: PMC12298743
- DOI: 10.3390/pharmaceutics17070943
Long-Term Effect of Semaglutide on the Glomerular Filtration Rate Slope in High-Risk Patients with Diabetic Nephropathy: Analysis in Real-World Clinical Practice
Abstract
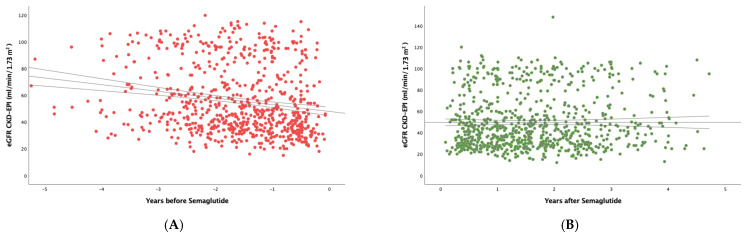
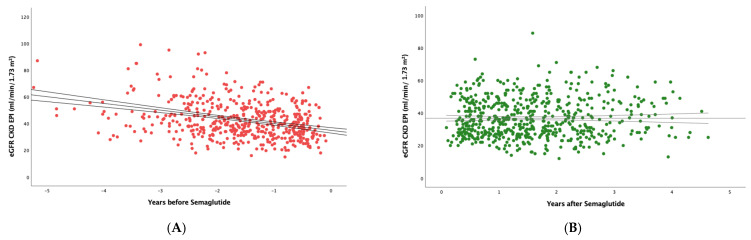
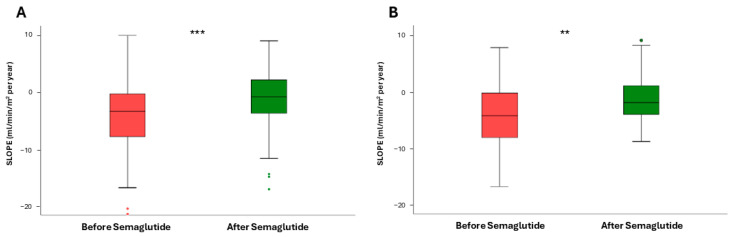
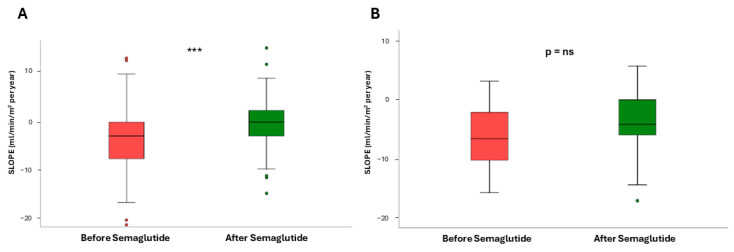
Background: Semaglutide, a GLP-1 receptor agonist, has shown promising nephroprotective effects in clinical trials, though real-world data on its long-term impact on renal function in high-risk diabetic nephropathy patients remain scarce. Methods: We conducted a multicenter, retrospective observational study involving 156 patients with type 2 diabetes and chronic kidney disease (CKD) treated with subcutaneous semaglutide between 2019 and 2023. Inclusion required an eGFR > 15 mL/min/1.73 m2 or albuminuria > 30 mg/g and at least two years of follow-up. The primary outcome was the change in eGFR slope after semaglutide initiation. Subgroup analyses were performed based on baseline eGFR, albuminuria, and SGLT2i co-treatment. Results: In the whole study population, the median eGFR slope significantly improved from -3.29 (IQR 7.54) to -0.79 (IQR 6.01) mL/min/1.73 m2/year post-treatment (p < 0.001). Multiple linear regression showed a hazard ratio for the effect of semaglutide on the eGFR slope of 4.06 (2.43-5.68), p < 0.001. In patients with baseline eGFR < 60 mL/min/1.73 m2, the slope improved from -3.77 to -1.01 (p < 0.0001), while patients on concurrent SGLT2i therapy saw slope changes from -2.96 to -0.37 (p < 0.0001). Patients with albuminuria 30-1000 mg/g also improved from -2.96 to -0.04 (p < 0.0001); however, those > 1000 mg/g did not show a significant change (p = 0.184). Semaglutide also reduced BMI (p = 0.04), HbA1c (p = 0.002), triglycerides (p = 0.001), CRP (p = 0.003), and GGT values (p = 0.004). Conclusions: In real-world practice, semaglutide significantly attenuated renal function decline in high-risk diabetic patients, particularly those with advanced CKD or concurrent SGLT2i therapy. These findings support its nephroprotective role beyond glycemic control.
Keywords: SGLT2 inhibitors; chronic kidney disease; diabetes; eGFR slope; estimated glomerular filtration rate; semaglutide.
Conflict of interest statement
Author Enrique Luna has received speaker honoraria and financial support for attending symposia from Novo Nordisk, Lilly, GSK and Esteve. The other authors declare that they have no conflict of interest. The companies had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Lewis E.J., Hunsicker L.G., Clarke W.R., Berl T., Pohl M.A., Lewis J.B., Ritz E., Atkins R.C., Rohde R., Raz I., et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N. Engl. J. Med. 2001;345:851–860. doi: 10.1056/NEJMoa011303. - DOI - PubMed
-
- Heerspink H.J.L., Jongs N., Chertow G.M., Langkilde A.M., McMurray J.J.V., Correa-Rotter R., Rossing P., Sjöström C.D., Stefansson B.V., Toto R.D., et al. Effect of dapagliflozin on the rate of decline in kidney function in patients with chronic kidney disease with and without type 2 diabetes: A prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021;9:743–754. doi: 10.1016/S2213-8587(21)00242-4. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
